Volume 1, Issue 9
December 2021
Negative Appendectomy after Histopathology: Results, Rates, and Predictive Factors
Sultan H. Alsaigh, Aishah S. Omar, Shahad S. Aljohani, Ebtesam A. Almadi, Ghayda S. Alwahbi, Hind K. Albahli, Asma A. Alsowiyan
DOI: http://dx.doi.org/10.52533/JOHS.2021.1902
Keywords: Negative appendectomy, acute appendicitis, Alvarado score
Background: Appendicitis is one of the most common causes of acute abdomen caused by an inflammation of the lining of the vermiform appendix. The management is usually emergent surgical removal. Histopathological examination of the appendectomy specimens are routinely carried out to correlate the histological findings of appendectomy specimens with the clinical diagnosis of acute appendicitis.
Methods: This is a retrospective chart review study that utilized the medical records of patients who underwent appendectomy from January 1, 2016 to March 31, 2019 in King Fahad Specialist Hospital (KFSH) in Buraidah.
Results: Negative Appendectomy (NA) rate in our study was 7.2% of total 488 patient. According to our findings, a positive computed tomography (CT) was the sole independent predictor of the absence of NA. The prevalence of NA increased among patients with negative CT, an Alvarado score ? 4 and those with an illness duration >1 day.
Conclusions: Appendicitis can be challenging to diagnose, and misdiagnosis was mostly associated with female gender. To reduce NA rate, CT scans can be used for patients with symptoms of acute appendicitis and the improvement of the Alvarado score. Further prospective studies are needed to validate our findings and demonstrate how unnecessary appendectomies can be avoided.
Introduction
Acute appendicitis (AA) is the most common cause of acute abdomen requiring emergent surgery (1). The exact etiology of AA remains uncertain but it is believed that it is mainly caused by an obstruction of the appendix lumen leading to luminal blockage by goblet cell secretions, which increase appendix wall pressure. The increased wall pressure may cause ischemia and the translocation of bacteria through the compromised mucosa, resulting in transmural inflammation. Tissue ischemia and inflammation can eventually cause complications, such as infarction and perforation of the appendix (2). The prevalence rate of AA was found to be 29.8% (range: 6.4% – 75.4%) in 2017 (3). Moreover, in a more recent study, the prevalence of AA was higher in men (62.6%) than in women (37.6%) (4). Although a wide range of clinical presentations are associated with AA, right iliac fossa pain, guarding, migratory periumbilical pain, and fever strongly suggest AA in adults (5,6). Contrarily, if vomiting precedes abdominal pain, appendicitis is less likely to be present (5).
Several scoring systems for diagnosing AA are available. These include Alvarado scoring system, which is based on patient history, clinical examination, and white blood cell count (1). Computed tomography (CT), ultrasound (US) imaging, and inflammatory markers such as C-reactive protein can be used to exclude AA. Other disorders may mimic AA such as gastroenteritis, Meckel’s diverticulitis, infectious colitis, Crohn’s disease, mesenteric adenitis, renal colic, and renal infarction (1,7-9). Moreover, the differential diagnosis in female patients is broad, including conditions such as ectopic pregnancy, pelvic inflammatory disease, ovarian torsion and endometriosis (7). Histopathology of appendectomy specimens confirm the diagnosis of AA. Specimens typically show fecaliths or worms, neurogenous hyperplasia, appendiceal neuroma, granulomatous inflammation, foreign body reaction, mucocele, endometriosis, cystadenoma, or appendiceal tumors (10). Additionally, the gold standard management for uncomplicated appendicitis is usually surgery. There are two main treatment approaches for appendectomy: open surgery and laparoscopic surgery. Many studies have shown that the laparoscopic approach has many advantages over open surgery. Those advantages include reduced incidence of surgical site infection, short hospital stay, lower risk of postoperative bowel obstruction, early return to work, early resumption of oral feeding, and lower risk of incisional hernias (11). On other hand Common adverse outcomes of appendectomy are surgical wound infection and intra-abdominal complications, which are associated with older age and perforated appendicitis (12). In addition, conservative treatment with antibiotics played an important role in the management of appendicitis with abscess or phlegmon (13). Delay in intervention can lead to complications such as peri-appendicular abscess formation and intra-abdominal adhesion, or even perforation (14,15). Fear of delayed diagnosis related complications have led to the removal of uninflamed appendixes which is known as negative appendectomy (NA) (1). Several factors are associated with NA, including female gender, especially among women of reproductive age, normal white blood cell count, normal C-reactive protein level, and CT unavailability. However, recently, NA rate has decreased with the routine use of CT and Alvarado scoring in patients with appendicitis (1,16). The estimated rate of NA varies from 4% – 45 %, with the highest incidence in women of reproductive age (16). We aim to measure the rate at which NA is performed after the availability of histopathological examination results by reviewing the medical records?
Methods
We performed a retrospective chart review study, using the medical records of patients who underwent appendectomy from January 1, 2016 to March 31, 2019 in King Fahad Specialist Hospital (KFSH). We included patients who underwent non-interval and non-incidental appendectomies during other surgeries involving the abdomen, regardless of age and gender. Collectively, the number of patients who met the inclusion criteria was (508). Patients who did not have a final histopathology report were excluded. We reviewed the history, physical examination findings, investigations, operative report, course of admission and final histopathology reports of the included patients. Each patient was given a number, from 1 to 508, for anonymization. All data were analyzed using the Statistical Package for the Social Science software, version 20 (Windows evaluation version). Final histopathology results were compared to the different characteristics of the patients by using Chi-square test and a logistic regression module was applied. Statistical significance was set at P-value of 0.5.
Results
This study analyzed 508 patients who were diagnosed with appendicitis, and we excluded 20 patients because of the data shortage in their medical records. The most common age group was 18 – 25 years, two-third of patients (66.6%) were male and the majority were Saudi nationals (81.6%). With respect to their marital status, the majority of patients (73%) were single. The prevalence of NA patients was 7.2% (35 patients), while positive appendectomy patients composed 92.8% (452 patients) of the cohort. Furthermore, the proportion of patients with associated comorbidities was 18% (Table 1).
|
Table 1: Baseline Characteristics of the patients (n=488) |
|
|
Study data |
N (%) |
|
Age group in years |
|
|
115 (23.6%) |
|
164 (33.6%) |
|
132 (27.0%) |
|
77 (15.8%) |
|
Gender |
|
|
325 (66.6%) |
|
163 (33.4%) |
|
Nationality |
|
|
398 (81.6%) |
|
90 (18.4%) |
|
Marital status |
|
|
356 (73.0%) |
|
132 (27.0%) |
|
Histopathology |
|
|
35 (07.2%) |
|
453 (92.8%) |
|
Comorbidities |
|
|
88 (18.0%) |
|
400 (82.0%) |
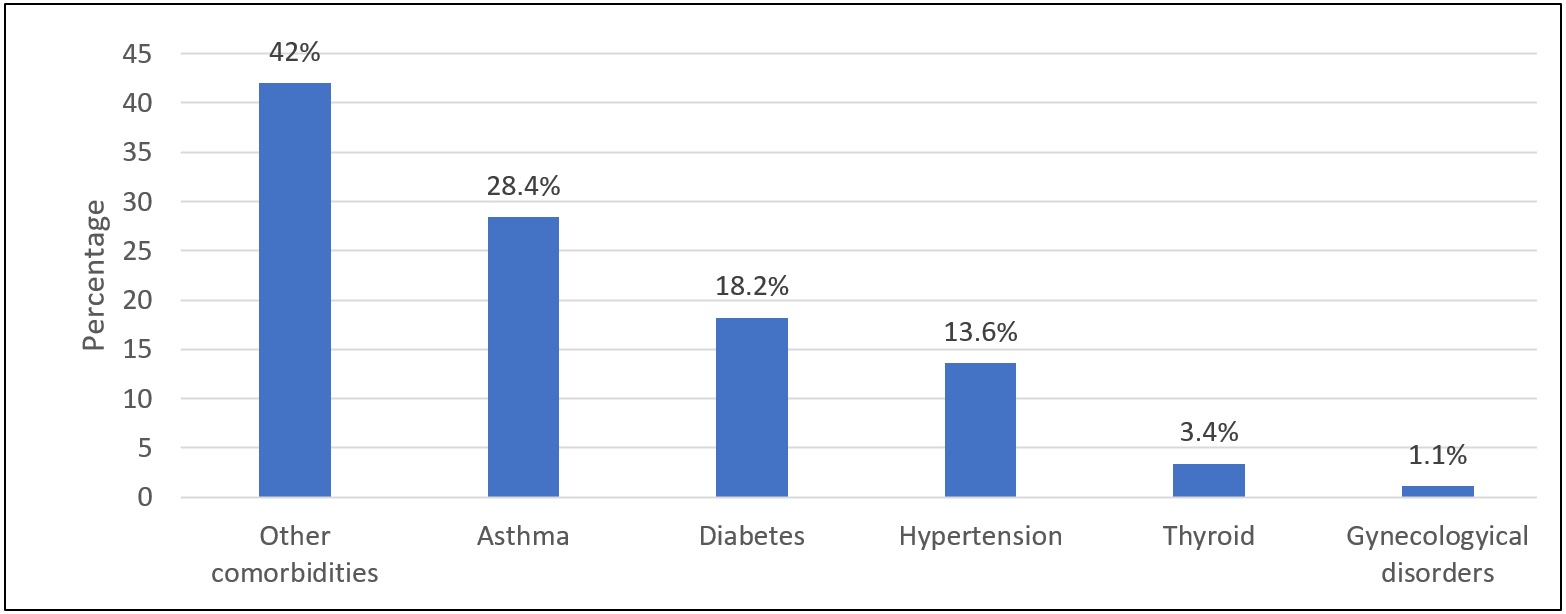
It can be observed that the most commonly known associated comorbidity was asthma (28.4%), then diabetes (18.2%) and hypertension (13.6%) while the least of them was gynecological disorder (1.1%) (Figure 1).
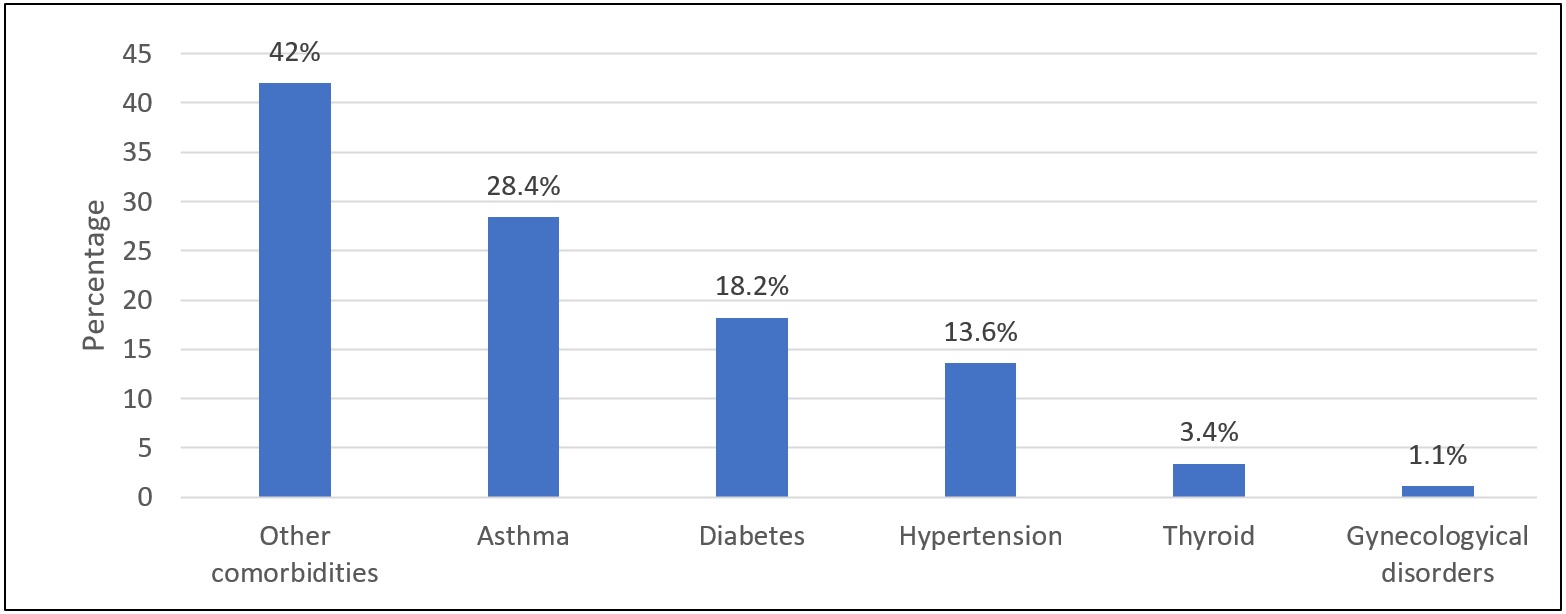
Figure 1: Associated comorbidities of the included patients
According to the results, the most frequently reported signs of appendicitis were right iliac fossa tenderness (80.3%) and rebound tenderness (56.8%). Regarding symptoms, the most common symptoms were nausea (63.1%), vomiting (55.7%) and anorexia (41.2%); while diarrhea (1.8%) was the least common. The proportion of patients with a leukocyte count ?10,000 was 95.3%, while the patients with left shift (Neutrophil ?75%) was 95.1%. Approximately 60% of patients had an Alvarado score of 5 –7, 24.2% had a score ? 4 and 17.6% had a score ? 8. Similarly, 11.5% of patients were negative for appendicitis via ultrasound, whereas 79.09% were classed as positive for appendicitis via CT. Additionally, 61.8% of patients were reported to have an illness duration of ?1 day, although 35% of patients reported a duration of >1 day. The proportion of patients who had been prescribed antibiotics was 95.7% (Table 2).
|
Table 2: Signs, symptoms, laboratory findings, imaging results and treatment of the patients (n=488) |
|
|
Variables |
N (%) |
|
Signs * |
|
|
16 (03.3%) |
|
11 (02.3%) |
|
392 (80.3%) |
|
277 (56.8%) |
|
Symptoms * |
|
|
201 (41.2%) |
|
308 (63.1%) |
|
272 (55.7%) |
|
09 (01.8%) |
|
172 (35.2%) |
|
Leukocytes |
|
|
465 (95.3%) |
|
23 (04.7%) |
|
Left shift |
|
|
464 (95.1%) |
|
24 (04.9%) |
|
Alvarado score |
|
|
118 (24.2%) |
|
284 (58.2%) |
|
86 (17.6%) |
|
Ultrasound |
|
|
56 (11.5%) |
|
29 (05.9%) |
|
403 (82.6%) |
|
CT scan |
|
|
09 (01.8%) |
|
390 (79.9%) |
|
89 (18.2%) |
|
Duration of illness (n=448) |
|
|
277 (61.8%) |
|
157 (35.0%) |
|
14 (03.1%) |
|
Use of antibiotics |
|
|
467 (95.7%) |
|
21 (04.3%) |
* Variable with multiple responses.
A Chi-square test was used to determine the relationship between appendectomy and socio-demographic and other related characteristics of the patients. The results showed that the prevalence of NA was higher among patients with an Alvarado score ? 4 (p<0.001), those with a negative CT (p<0.001) and those with an illness duration >1 day (p=0.001). Meanwhile, the prevalence of NA was significantly less frequent among males (p=0.048). However, the relationship between appendectomy and age group (p=0.997), nationality (p=0.510), marital status (p=0.163), comorbidities (p=0.124), ultrasound findings (p=0.608), and use of antibiotics (p=0.193), was not significant (Table 3).
|
Table 3: Relationship between histopathology among the Baseline Characteristics, treatment and imaging results of the patients (n=488) |
|||
|
Factor |
Appendectomy |
P-value § |
|
|
Negative N (%) (n=35) |
Positive N (%) (n=453) |
||
|
Age group in years |
|||
|
20 (07.2%) |
259 (92.8%) |
0.997 |
|
15 (07.2%) |
194 (92.8%) |
|
|
Gender |
|||
|
18 (05.5%) |
307 (94.5%) |
0.048 ** |
|
17 (10.4%) |
146 (89.3%) |
|
|
Nationality |
|||
|
30 (07.5%) |
368 (92.5%) |
0.510 |
|
05 (05.6%) |
85 (94.4%) |
|
|
Marital status |
|||
|
22 (06.2%) |
334 (93.8%) |
0.163 |
|
13 (09.8%) |
119 (90.2%) |
|
|
Comorbidities |
|||
|
03 (03.4%) |
86 (96.6%) |
0.124 |
|
32 (08.0%) |
367 (92.0%) |
|
|
Alvarado score |
|||
|
18 (15.3%) |
100 (84.7%) |
<0.001 ** |
|
16 (05.6%) |
268 (94.4%) |
|
|
01 (01.2%) |
85 (98.8%) |
|
|
Ultrasound (n=85) |
|||
|
08 (14.3%) |
48 (85.7%) |
0.608 |
|
03 (10.3%) |
26 (89.7%) |
|
|
CT scan (n=399) * |
|||
|
05 (55.6%) |
04 (44.4%) |
<0.001 ** |
|
26 (06.7%) |
364 (93.3%) |
|
|
Duration of illness (n=448) * |
|||
|
10 (03.6%) |
267 (96.4%) |
0.001 ** |
|
20 (11.7%) |
151 (88.3%) |
|
|
Use of antibiotics |
|||
|
35 (07.5%) |
432 (92.5%) |
0.193 |
|
0 |
21 (100%) |
|
* Not done were excluded from the analysis, § P-value has been calculated using Chi-square test., ** Significant at p<0.05 level.
A multivariate regression analysis was subsequently performed to determine the independent significant predictor associated with NA. The results, revealed that NA was significantly less in patients with a positive CT result (AOR=0.065; 95% CI=0.012 – 0.342; p=0.001). Thus, a positive CT was the sole independent predictor inversely associated with NA. Other variables included in the model such as gender, Alvarado score, and duration of illness did not show significant effect after adjustments to the regression model (p>0.05) (Table 4).
|
Table 4: Determining the factor associated with negative appendectomy (n=488) |
|||
|
Factor |
AOR |
95% CI |
P-value |
|
Gender |
|||
|
Ref |
||
|
1.323 |
0.557 – 3.141 |
0.526 |
|
Alvarado score |
|||
|
Ref |
||
|
0.166 |
0.020 – 1.355 |
0.094 |
|
0.3530 |
0.044 – 2.804 |
0.325 |
|
CT scan (n=399) * |
|||
|
Ref |
||
|
0.065 |
0.012 – 0.342 |
0.001 ** |
|
Duration of illness (n=448) * |
|||
|
Ref |
||
|
2.371 |
0.965 – 5.829 |
0.060 |
AOR – Adjusted Odds Ratio; CI – Confidence Interval, * Not done were excluded from the analysis, ** Significant at p<0.05 level.
Discussion
According to a Shchatsko et al, AA is the most common indication for surgery (17). The similarity of symptoms between appendicitis and other conditions have led to NA cases. A patient is exposed to needless surgery and anesthesia when an uninflamed appendix is removed (16). Our study showed similar results to two retrospective studies which were done by Alhamdani et al. in 2018 and Seetahal et al in 2007 respectively. The authors in both studies found a NA rate of 9.5% compared to 7.2% which was reported in our study (1,18). Several studies have shown that NA incidence is higher in women of reproductive age than in women of other ages, which seemed to be related to diagnostic challenges and confusion with gynecological disorders (16). Our study also revealed a significant occurrence of NA in women. However, we did not find a significant association between appendectomy and age.
The Alvarado score is a predictive score for AA that utilize history, laboratory results and clinical findings (19). In the Alvarado scoring system, a score of 1– 4 indicates a low probability of AA, a score of 5–6 indicates probable AA, and a score of 7–10 indicates that the appendix is most probably inflamed (20). In this study, approximately 60% of patients had an Alvarado score of 5–7, 24.2% had a score of ?4, and 17.6% of patients had a score of ?8. The research results indicate that patients who had scores of ?4 were at a higher risk of NA. Multivariate regression analysis for the Alvarado score showed an insignificant effect, after adjustments for the regression model. Thus, the Alvarado score may have a positive impact on NA assessment but further modifications may be required. There are controversies regarding the relationship between CT use and NA prevalence (21,22). A retrospective study done in 2005 for 753 patients
demonstrated no decrease in NA rates following the introduction of CT and US (22). Contrarily, a retrospective study done in 2004 for 394 patients indicated improvement in NA rate with application of CT. According to the results of our study, NA was significantly less likely in patients who had a positive CT. Thus, a positive CT was the only independent predictor of the absence of NA. We also found that the majority of patients in our hospital (93.5%) that were scheduled for appendectomy underwent CT. Our data also suggests that the use of CT may have resulted in decreased NA prevalence. However, in line with the results of a study by Giljaca V et al, US seemed unreliable in assessing NA as they found sensitivity and specificity of US for diagnosis of AA were 69% and 81%, respectively (23). However, US was not performed in most patients (only 82 patients, 6%); thus, we can only make speculations (24).
The most common symptom in our patients was nausea (63.1%), vomiting (55.7%), anorexia (41.2%), and diarrhea (1.8%). These findings are similar to those of a study by Joshi et al, as they noticed that vomiting is reported by 59.1 % of cases and diarrhea reported by 11 cases (16). The authors observed anorexia in 70 % of cases and vomiting and fever in 59.1% and 45.7% of cases, respectively. They also reported other symptoms, including diarrhea, constipation and dysuria. In our study, asthma was the most common comorbidity, followed by diabetes and hypertension, while the least common was gynecological disorder. None of these comorbidities had a significant association with NA. By comparing the duration of illness, we found that NA prevalence was significantly higher among those with an illness duration of >1 day. However, our illness duration outcomes did not show a predictive association with NA. Our study had several limitations. Most patients (two-thirds) were male; thus, the study sample is not representative of the female population. Finally, our findings may not be generalizable since our sample population was derived from one hospital.
Conclusion
Appendicitis can be challenging to diagnose. The NA rate in our study was 7.2%, and misdiagnosis was mostly associated with females. A positive CT was the sole independent predictor of the absence of NA. To reduce NA rate, we suggest the utilization of CT for patients with symptoms of AA and the improvement of the Alvarado score. Further prospective studies are needed to validate our findings and demonstrate how unnecessary appendectomies can be avoided.
Acknowledgements
We thank Rana Alhammad, Montaha Almohaimeed, and Raghad Alkhudair for their efforts in data collectection. We thank KFSH for providing the data for this research.
Disclosure
Statement:
This material is the authors' own original work in a truthful and complete manner which has not been previously or currently being considered for publication elsewhere. The results are appropriately placed in the context of prior and existing research. Furthermore, the authors declare no conflict of interest.
Funding:
None.
Ethical consideration:
Ethical approval was obtained (No. 1441-2157833) for implementation and publication of this study from Dr Abdullah M. Al Saigul Chairman of Research Ethics Committee at Qassim Province. Patient data were collected without personal identifiers. Adequate level of confidentiality of the research data had been ensured.
Data availability:
Data that support the findings of this study are available from KFSH. Data is available from the authors upon reasonable request and with permission of KFSH.
Author Contribution:
SHA, ASO and AAA conceived and designed the study, conducted research, provided research materials. SSA and HKA analyzed and interpreted data. EAA, GSA wrote initial and final draft of article, and provided logistic support. All authors have collected, organized data, and critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.