Volume 6, Issue 5
May 2026
Effect of Screen Time, Sedentary Behavior, and Sleep Disruption on Obesity and Metabolic Syndrome in Adolescents and Young Adults: A Systematic Review
Zinat Mohamed Abdel Fattah, Siddiqa Mohamed Ali, Amal Muhaysin Alruwaili, Sara Ali Alqurus, Noha Hassan Qummosani
DOI: http://dx.doi.org/10.52533/JOHS.2026.60503
Keywords: obesity, sedentary behavior, sleep patterns, metabolic syndrome, screen time, leisure time
Background: The prevalence rates of overweight and obesity are witnessing a significant rising trend among adolescents and young adults. One in five children is considered overweight, with an overall prevalence of obesity recorded at 8.5%. Additionally, about 25% of the world’s population is diagnosed with metabolic syndrome. Young adults and adolescents are at higher risk of developing metabolic syndromes, making them susceptible to developing cardiovascular diseases. Sedentary behavior increases the risk of mortality, cardiovascular diseases, diabetes mellitus, hypertension, and metabolic syndrome. This systematic review aims to evaluate the association between screen time, sedentary behavior, and sleep disruption with obesity and metabolic syndrome among adolescents and young adults.
Methodology: This systematic review was conducted according to the PRISMA checklist. Major outcomes included the associations between screen time, smartphone use, sleep duration, sedentary behavior, and physical activity with obesity-related and cardiometabolic outcomes across children, adolescents, and young adults. A comprehensive search was conducted using a combination of electronic databases, including PubMed, Scopus, and Web of Science.
Results: The review included 14 observational studies, published between 2010 and 2025. The findings of the included studies demonstrated that higher screen time, sedentary behavior, poor sleep duration, and lower physical activity levels were associated with adverse obesity-related and cardiometabolic outcomes. Multiple studies reported that prolonged screen exposure was significantly associated with higher BMI, abdominal obesity, metabolic syndrome, central adiposity, elevated triglycerides, and reduced cardiorespiratory fitness. Short sleep duration was associated with higher obesity risk, increased insulin resistance, and elevated fasting insulin levels. Physical activity demonstrated a generally protective association against obesity and metabolic abnormalities.
Conclusion: Modifiable lifestyle-related habits such as excessive screen time, sedentary behavior, and inadequate sleep duration are associated with adverse obesity and cardiometabolic outcomes among adolescents and young adults. Therefore, reducing recreational screen exposure, improving sleep hygiene, and promoting regular physical activity should represent important public health priorities.
Introduction
Recent global trends have shown a significant rise in the rates of overweight and obesity among adolescents and young adults. The World Health Organization (WHO) defines Obesity as a Body Mass Index (BMI) of 30 kg/m² or higher and is categorized as class 1 (30·0–34·9 kg/m²), class 2 (35·0–39·9 kg/m²), and class 3(≥40·0 kg/m²) (1). In 2022, the WHO reported that approximately 37 million children under the age of 5, in addition to over 390 million children and adolescents aged between 5 and 19 years, were either overweight or living with obesity (2). Furthermore, a recent study reported that one in five children is considered overweight, with an overall prevalence of obesity recorded at 8.5% (3). Additionally, the highest prevalence of obesity was reported among Hispanic and black youth populations (3).
Metabolic syndrome is an asymptomatic, pathophysiological state characterized by a group of interrelated metabolic abnormalities, including obesity, insulin resistance, hypertension, dysglycaemia, and dyslipidaemia (4). Individuals diagnosed with metabolic syndrome often present with a large waist circumference, elevated triglycerides, low levels of high-density lipoprotein (HDL) cholesterol, elevated blood pressure, and elevated fasting blood glucose (5). Recent estimates report that approximately 25% of the world’s population is diagnosed with or affected by metabolic syndrome; moreover, the prevalence rates vary depending on age, gender, and ethnicity (6). Additionally, young adults are at higher risk of developing metabolic syndromes, rendering them at high risk of developing cardiovascular diseases as well (4).
Sedentary behavior is defined as any waking behavior with an energy expenditure of 1.5 metabolic equivalent task or less (7). Sedentary behavior encompasses a group of behaviors that contribute to a lifestyle of inactivity (7). Such behavior increases the risk of mortality, cardiovascular diseases, diabetes mellitus, hypertension, cancer, and metabolic syndrome. Sedentary behaviors are significantly high among children, adolescents, and young adults. This population is often exposed to environments promoting inactivity through the excessive use of electronic devices.
The increased use of electronic devices leads to poor eye health and increases the risk of several chronic diseases, such as hypertension and diabetes mellitus, in addition to obesity and metabolic syndromes (8). Studies report that sedentary behaviors and high screen time are associated with an increased risk of metabolic syndrome among adolescents and young adults, and that the modifications of lifestyle help in the prevention and management of metabolic syndrome (9). Moreover, sleep disturbances have also been associated with obesity and metabolic syndrome among young adults and adolescents (10). Sleep disturbances, such as intermittent sleep and sleep deprivation, can result in dysregulation of the metabolic processes and cause hormonal imbalance, leading to obesity and the development of metabolic syndrome (10). This systematic review aims to systematically evaluate the association between screen time, sedentary behavior, and sleep disruption with obesity and metabolic syndrome among adolescents and young adults.
Methodology
Reporting Guidelines
The results were reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Outcome Definition and Eligibility Criteria
Major outcomes of interest included the associations between screen time, smartphone use, sleep duration, sedentary behavior, and physical activity with obesity-related and cardiometabolic outcomes across children, adolescents, and young adults. The search strategy of this systematic review was developed based on the Population, Intervention, Comparison, and Outcomes (PICO) framework and the study designs. The target population was children, adolescents, and young adults of any sex diagnosed with obesity or metabolic syndrome. Eligible interventions comprised increased smartphone use, reduced sleep duration, sedentary behavior, and physical inactivity. Comparator groups included lower smartphone use, adequate sleep duration, and increased physical activity.
Single case reports, or case series, editorials, commentaries, expert opinions without primary data, conference abstracts without full text, and narrative reviews were excluded. Additionally, Studies with insufficient or unclear data regarding outcomes, laboratory studies, posters, protocols, and articles not published in English were excluded as well.
Information Sources
A comprehensive search for a systematic review of the effect of screen time, sleep disruption, and sedentary behavior on obesity among adolescents and young adults, using a combination of electronic databases, including PubMed, Scopus, and Web of Science. The search strategy employed a combination of keywords and Medical Subject Headings (MeSH) related to the PICO framework. Keywords or search terms were combined using Boolean operators (AND/OR) to capture relevant studies.
Search Strategy
PubMed: (("Adolescent"[MeSH] OR "Young Adult"[MeSH] OR adolescent* OR youth OR teenager* OR "young adult*") AND ("Screen Time" OR "screen exposure" OR "digital media use" OR "television" OR "computer use" OR "smartphone use") AND ("Sedentary Behavior"[MeSH] OR sedentary OR "physical inactivity" OR "sitting time") AND ("Sleep"[MeSH] OR "sleep deprivation" OR "sleep disturbance*" OR "sleep duration" OR insomnia) AND ("Obesity"[MeSH] OR obesity OR overweight OR "body mass index" OR BMI OR adiposity) AND ("Metabolic Syndrome"[MeSH] OR "metabolic syndrome" OR "insulin resistance" OR dyslipidemia OR hypertension)).
Science direct: ("screen time") AND ("sedentary behavior") AND ("sleep disruption") AND (obesity OR "metabolic syndrome") AND (adolescents OR "young adults").
Cochrane: (screen time OR digital media OR television OR smartphone) AND (sedentary behavior OR physical inactivity OR sitting) AND (sleep disturbance OR sleep deprivation OR sleep duration) AND (obesity OR overweight OR BMI OR "metabolic syndrome") AND (adolescent OR youth OR "young adult").
Study Selection and Data Extraction
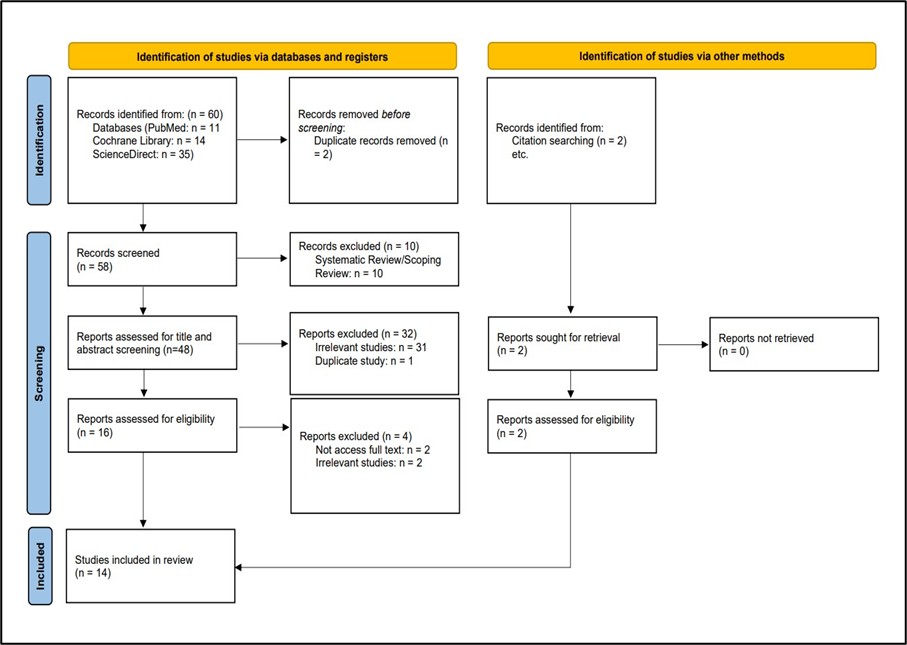
All records identified through the database search were imported into reference management software (EndNote X8), and duplicates were removed. Two reviewers independently screened titles and abstracts for eligibility. Full-text articles were then retrieved and assessed independently by the same reviewers against the predefined inclusion and exclusion criteria. Disagreements at any stage of the screening process were resolved through discussion and, when necessary, consultation with a third reviewer. The study selection process was documented using a PRISMA flow diagram (Figure 1).
Data was independently extracted by two reviewers using a standardized data extraction form. Extracted information included study characteristics (author, year, country, and study design), participant characteristics (gender and age of the study population), and key findings related to screen time, sedentary behavior, sleep disturbances, and their association with obesity and overweight. Any discrepancies in data extraction were resolved by consensus.
Quality Assessment
The methodological quality and risk of bias of the included studies were assessed using established assessment tools. The Newcastle-Ottawa Scale (NOS) was used for observational studies, including cohort and case-control designs (11). The assessment focused on methodological aspects such as study design, sample size, data collection methods, and risk of bias.
Results
Search results
The initial search found 60 articles. After removing duplicates and screening titles, abstracts, and full texts, the search was narrowed to 12 studies. Two studies were identified through a manual search. Finally, 14 studies were included in this study. Figure 1 shows the study selection process.
Figure 1: PRISMA flow chart
Characteristics of the Included Studies
Fourteen studies met the inclusion criteria, published between 2010 and 2025 in different countries such as the USA, Brazil, Indonesia, Kuwait, Saudi Arabia, UAE, China, and India. All the studies included were observational studies. Most study designs were cross-sectional, with a few cohort study designs. The included studies collectively evaluated the associations between screen time, smartphone use, sleep duration, sedentary behavior, and physical activity with obesity-related and cardiometabolic outcomes across children, adolescents, and young adults. Sample sizes ranging from 120 obese adolescents with metabolic syndrome to large population-based cohorts involving 58,712 participants. Many studies focused on school-aged children and adolescents, while a few included university students and young adults aged 18–25 years. Both sexes were represented across studies. Table 1 summarizes the key details of the studies included in this meta-analysis (Table 1).
|
Table 1: Baseline Characteristics of included studies |
||||||
|
Study |
Country |
Study Design |
Population/Setting |
Age Group (Mean/range) |
Sample Size |
Female/Male (%) |
|
Alexander et al., 2025 (18) |
USA |
Longitudinal observational |
Adolescents from ABCD study |
Mean 14.1 years |
791 |
53%/47% |
|
Al-Hazzaa & Albawardi, 2019 (15) |
Saudi Arabia |
Cross-sectional |
Secondary school students |
15–19 years |
2888 |
51.94%/48.06% |
|
Alkatan et al., 2021 (20) |
Kuwait |
Cross-sectional |
Physical education college students |
20.8 ± 2.3 |
418 |
52.63%/47.37% |
|
Al-Shoaibi et al., 2026 (24) |
USA |
Prospective cohort |
Adolescents with overweight/obesity |
9–11 years |
3498 |
45.11%/54.89% |
|
Cheng et al., 2024 (8) |
China |
Cross-sectional |
Children and adolescents |
7–17 years |
58,712 |
49.99%/50.01% |
|
Khan et al., 2019 (17) |
UAE |
Cross-sectional |
Expatriate school adolescents |
14.9 ± 1.9 |
474 |
47.1%/52.90 |
|
Riyas Basheer et al., 2025 (19) |
India |
Cross-sectional |
Smartphone-using young adults |
20.42 ± 1.64 |
200 |
50%/50% |
|
Sehn et al., 2024 (12) |
Brazil |
Longitudinal study |
Schoolchildren and adolescents |
6–17 years |
331 |
57.7%/42.30 |
|
Shan et al., 2010 (21) |
China |
Cross-sectional |
Community children/adolescents |
2–18 years |
21,198 |
50%/50% |
|
Vella et al., 2020 (14) |
USA |
Cross-sectional |
College-aged adults |
Mean 19.9 years |
95 |
59%/41% |
|
Moitra et al., 2021 (13) |
India |
Cross-sectional |
Adolescents |
10–15 years |
722 |
52.35%/47.65% |
|
Pitanga et al., 2019 (16) |
Brazil |
Cross-sectional |
Adolescents |
15-18 years |
613 |
55.14%/44.86% |
|
Kurube et al., 2023 (22) |
Indonesia |
Cross-sectional |
Adolescents |
13–18 years |
120 |
32.5%/67.5% |
|
Fernanda Rocha de Faria et al., 2025 (23) |
Brazil |
Cross-sectional study |
Adolescents |
15–18 years |
349 |
48.42%/51.58 |
Outcome Measures of the Included Studies
The exposure variables in the included studies primarily consisted of screen time, sleep duration, smartphone addiction or use, sedentary behavior, and physical activity levels. In studies, screen exposure was classified mainly using time cutoffs of ≥2 hours/day or ≥3 hours/day; however, sleep duration was commonly assessed against recommended sleep thresholds of 8–11 hours/day. Physical activity was assessed as a leisure-time activity, using minutes/week, or moderate-to-vigorous physical activity measures. Some studies included additional factors such as dietary behaviors, including fast-food intake, sugar-sweetened beverages, and snack consumption, as covariates or related lifestyle behaviors. The major outcome measures of the included study were primarily obesity-related and cardiometabolic indicators, including BMI, waist circumference, waist-to-height ratio, body fat percentage, metabolic syndrome (MetS), insulin resistance, blood pressure, lipid profiles, triglycerides, HDL-C, and clustered cardiometabolic risk scores.
The findings of the included studies consistently demonstrated that higher screen time or higher leisure screen time, sedentary behavior, poor sleep duration, and lower physical activity levels were associated with adverse obesity-related and cardiometabolic outcomes. Multiple studies reported that prolonged screen exposure was significantly associated with higher BMI (12-14), abdominal obesity (8, 15, 16), metabolic syndrome (8, 17), central adiposity (13), elevated triglycerides (8, 14), and reduced cardiorespiratory fitness (14). Large population-based studies by Cheng et al (8) reported that adolescents with higher sedentary time and screen exposure Screen time ≥3 h/day was associated with higher odds of abdominal obesity (OR = 1.15, 95% CI: 1.08–1.22) and MetS (OR = 1.14, 95% CI: 1.03–1.25). Similarly, smartphone addiction and excessive smartphone use explored by Alexander et al. (18) and Riyas Basheer et al. 2025 (19) found that it was associated with poorer sleep quality, increased BMI, sedentary behavior, elevated psychological distress, and unfavorable anthropometric and blood pressure measures.
Sleep duration emerged as an important protective factor in most of the studies. Short sleep duration was consistently associated with higher obesity risk, increased insulin resistance, elevated fasting insulin levels, and reduced likelihood of transitioning from overweight/obesity to normal BMI percentile (12, 15, 18, 20-23). Longitudinal evidence further indicated that inadequate sleep and increased screen exposure may contribute to persistent cardiometabolic risk over time (Table 2).
|
Table 2: Key Findings of the included studies |
|||
|
Study |
Exposure Variable |
Outcome Measure |
Key Findings |
|
J. D. Alexander et al. (18) |
Smartphone use (daytime/evening, late-evening, late-night use) |
Sleep duration, sedentary behavior, physical activity |
Late-night smartphone use was associated with reduced sleep duration, delayed sleep onset/waking time, increased sedentary behavior, and fewer daily steps (standardized β = −0.16 to −0.27, p < 0.001). Daytime/evening use was associated with reduced exercise and increased sedentary behavior (β = −0.21 to −0.07, p < 0.001). |
|
Al-Hazzaa & Albawardi, 2019 (15) |
Screen time, physical activity, sleep duration |
Sedentary behavior, sleep duration, obesity indicators |
Higher screen time (>3 h/day) was associated with reduced sleep duration and fast-food intake (p < 0.001). Active males had lower abdominal obesity than inactive males (WHtR ≥0.50: 33.3% vs 39.2%, p = 0.014). Total activity energy expenditure and sum of vigorous-intensity physical activity showed significant interaction effects between gender and obesity status, whereas sum of moderate activity energy expenditure, non-leisure-time physical activity and sleep duration exhibited significant interaction effects between gender and screen time |
|
Alkatan et al., 2021 (20) |
Physical activity level, screen time, sleep duration |
Physical activity expenditure, sedentary behavior, obesity/fat percentage |
High physical activity (>600 METs-min/week) was reported in 87.9% of participants, with males more active than females (96.0% vs 80.8%, p < 0.005). Mean screen time was high (5.55 ± 0.15 h/day), with 76.8% exceeding 3 h/day. Higher activity levels (>1200 METs-min/week) were associated with lower obesity-level body fat percentage (40.2% vs 54.2%, p = 0.012). Lower screen time (<3 h/day) was inversely associated with high activity levels (aOR = 0.517, 95% CI: 0.279–0.958, p = 0.036). |
|
Cheng et al. (8) |
Sedentary time, screen time, physical activity |
MetS and MetS components |
High sedentary time was associated with abdominal obesity (OR = 1.41, 95% CI: 1.31–1.52), high triglycerides (OR = 1.16, 95% CI: 1.08–1.25), low HDL-C (OR = 1.12, 95% CI: 1.03–1.22), and MetS (OR = 1.35, 95% CI: 1.20–1.52). Screen time ≥3 h/day was associated with higher odds of abdominal obesity (OR = 1.15, 95% CI: 1.08–1.22) and MetS (OR = 1.14, 95% CI: 1.03–1.25). |
|
Al-Shoaibi et al., 2026 (24) |
Sleep duration, screen time, physical activity |
Transition from overweight/obesity to normal BMI percentile |
Adolescents sleeping 7–8 h/day were less likely to transition to normal BMI percentile compared with those sleeping 9–11 h/day (HR = 0.60, 95% CI: 0.44–0.82; p-trend = 0.003). Similar findings were observed in females (HR = 0.55, 95% CI: 0.30–0.98) and males (HR = 0.59, 95% CI: 0.41–0.86). Screen time was not significantly associated with BMI normalization (HR = 0.99, 95% CI: 0.96–1.02). |
|
Khan et al. (17) |
Screen time (computer, television, video games) |
MetS |
MetS prevalence was higher among adolescents reporting ≥2 h/day screen time compared with <2 h/day (13.5% vs 8.5%). Each additional hour of screen time increased the likelihood of MetS by 21% (OR = 1.21, 95% CI: 1.08–1.35). Adolescents with ≥2 h/day screen time had higher odds of MetS (adjusted OR = 2.20, 95% CI: 1.04–4.67). |
|
Riyas Basheer et al., 2025 (19) |
Smartphone addiction |
BMI, sleep quality, psychological distress, blood pressure |
Smartphone addiction scores were positively correlated with BMI, poorer sleep quality, higher psychological distress, and increased systolic/diastolic blood pressure (all p < 0.05). Mean PSQI score was 5.07 ± 2.99 and mean BMI was 21.19 ± 4.32 kg/m². |
|
Sehn et al., 2024 (12) |
Screen time, sleep duration, physical activity |
Clustered cardiometabolic risk score (cMetS) |
Higher screen time at baseline was associated with shorter sleep duration at follow-up (B=-0.074; 95%IC=-0.130; -0.012), while higher Z_BMI from baseline associated with higher cMetS of follow-up (B=0.154; 95%CI=0.083;0.226). The reciprocal model of relationships indicated that the variance of ST, sleep time, leisure PA, Z_BMI, and cMetS explained approximately 9%, 14%, 10%, 67% and 22%, respectively, of the model. Baseline BMI z-score significantly predicted follow-up cMetS. |
|
Shan et al., 2010 (21) |
Screen time, physical inactivity, sleep duration |
Overweight and obesity |
Screen time ≥2 h/day was significantly associated with higher odds of obesity. Physical inactivity, less sleep duration, higher consumption of alcohol, snack food and Western fast food and more screen time were associated with overweight and obesity (p< 0.05) |
|
Vella et al., 2021 (14) |
Leisure screen time |
Cardiometabolic risk factors |
Higher leisure screen time was independently associated with higher BMI, waist circumference, fat mass, triglycerides, and lower cardiorespiratory fitness (VO2peak) after adjustment for confounders. No consistent associations were observed with blood pressure or glucose. |
|
Moitra et al., 2023 (13) |
Physical activity, screen time, sleep quality |
Overweight, obesity, central adiposity |
High screen time (>2 h/day) was significantly associated with obesity and central adiposity. The clustering of low PA and poor sleep quality was associated with a higher risk of obesity in girls and of low PA and excess ST with higher BMI and WHtR in boys. Girls who reported clustering of all three unhealthy behaviors had 2.88 times higher odds of obesity and 1.81 times increased odds of having central adiposity. The odds of obesity were 2.10 times higher in boys reporting low PA and 4.13 times higher in those with low PA+ excess ST. |
|
Pitanga et al., 2019 (16) |
Physical activity, screen time, dietary behaviors |
Overweight and abdominal obesity |
Combined effects of physical activity and screen time were associated with being overweight mainly among boys. In boys, being physically active with short weekend screen time was inversely associated with overweight compared to low physical activity and long screen time (OR=0.31, 95% CI: 0.12–0.85). No significant associations were observed among girls. Screen time ≥4 hours/day and lower physical activity levels were linked with increased overweight risk. |
|
Kurube et al., 2023 (22) |
Sleep duration |
Insulin resistance, metabolic syndrome components |
Short sleep duration (<8 h/day) was associated with higher insulin resistance (HOMA-IR: r = −0.581, p < 0.001) and higher fasting insulin levels (r = −0.565, p < 0.0001) among obese adolescents with metabolic syndrome. |
|
Fernanda Rocha de Faria et al., 2025 (23) |
Screen time, MVPA, sedentary behavior, sleep duration |
Cardiometabolic risk factors |
High screen time (>4 h/day) increased the odds of belonging to the high cardiometabolic risk group (OR = 4.39, 95% CI: 1.64–11.07). Higher sedentary behavior and shorter sleep duration were also associated with higher cardiometabolic risk. |
Physical activity demonstrated a generally protective association against obesity and metabolic abnormalities. Higher levels of moderate-to-vigorous physical activity were associated with lower body fat percentage (20), reduced overweight prevalence (21), and improved cardiometabolic profiles (12). Pitanga et al., 2019 (16) highlighted the combined effects of lifestyle behaviors, showing that clustering of high screen time, low physical activity, and poor sleep quality substantially increased the risk of obesity. Additionally, Moitra et al., 2023 (13) observed that the clustering of low PA and poor sleep quality was associated with a higher risk of obesity, especially in girls, and of low PA and excess ST with higher BMI and WHtR in boys. Sex-specific differences were observed in several studies, with boys often demonstrating stronger associations between screen time and overweight, whereas girls exhibited greater susceptibility to clustered unhealthy lifestyle behaviors (Table 2).
Quality Assessment Results
The 14 included studies were observational studies. Cohort studies (Table 3) were assessed using NOS, while cross-sectional studies (Table 4) were assessed using the modified NOS for Cross-Sectional Studies. Based on this assessment, all 3 cohort studies were rated as high quality, 7 of the cross-sectional studies were rated as high quality, with the remaining 4 studies rated as moderate quality.
|
Table 3: Quality Assessment of Cohort Studies Using the Newcastle–Ottawa Scale (NOS) |
|||||
|
Study |
Selection (Max 4) |
Comparability (Max 2) |
Outcome (Max 3) |
Total Score (Max 9) |
Quality |
|
J. D. Alexander et al. 2025 (18) |
**** |
** |
*** |
9 |
Good |
|
Al-Shoaibi et al., 2026 (24) |
**** |
** |
*** |
9 |
Good |
|
Sehn et al., 2024 (12) |
**** |
** |
*** |
9 |
Good |
|
Table 4: Quality Assessment of Cross-Sectional Studies Using Modified Newcastle–Ottawa Scale for Cross-Sectional Studies |
|||||
|
Study |
Study Sample Selection (Max 2) |
Assessment of Exposure/Outcome (Max 4) |
Confounding Factors (Max 3) |
Total Score (Max 9) |
Quality |
|
Al-Hazzaa & Albawardi, 2019 (15) |
** |
**** |
** |
8 |
Good |
|
Alkatan et al., 2021 (20) |
** |
*** |
* |
6 |
Moderate |
|
Cheng et al. (8) |
** |
**** |
*** |
9 |
Good |
|
Khan et al. (17) |
** |
*** |
** |
7 |
Good |
|
Riyas Basheer et al., 2025 (19) |
* |
*** |
* |
5 |
Moderate |
|
Shan et al., 2010 (21) |
** |
*** |
** |
7 |
Good |
|
Vella et al., 2021 (14) |
** |
**** |
** |
8 |
Good |
|
Moitra et al., 2023 (13) |
** |
**** |
** |
8 |
Good |
|
Pitanga et al., 2019 (16) |
** |
*** |
* |
6 |
Moderate |
|
Kurube et al., 2023 (22) |
* |
*** |
* |
5 |
Moderate |
|
Fernanda Rocha de Faria et al., 2025 (23) |
** |
**** |
** |
8 |
Good |
Discussion
Being among the risk factors for stroke, type-2 diabetes, and non-alcoholic fatty liver disease. Obesity and metabolic syndrome pose persistent health challenges, particularly among those aged 15-24 years. Thus, identifying lifestyle-related risk factors that can be modified offers an opportunity to improve long-term cardiometabolic health and reduce disease burden. Despite the previous literature supporting the association between modifiable lifestyle-related factors such as excessive screen exposure, prolonged sedentary behavior, poor sleep quality, and inadequate physical activity, with obesity and metabolic dysfunction, findings remain inconsistent. Furthermore, the combined influence of these behavioral factors across different populations remains unknown. Owing to these inconsistent findings, this systematic review evaluated the effects of screen time, sedentary behavior, and sleep disruption on obesity and metabolic syndrome among adolescents and young adults. Among the main outcome measures, excessive screen time, prolonged sedentary behavior, shorter sleep duration, and lower physical activity levels were associated with adverse obesity and cardiometabolic outcomes in this age group.
Baseline characteristics of the included studies demonstrated considerable variability in geographic location, sample size, and study design. Nevertheless, the included populations were generally homogeneous in age, as most studies evaluated school-aged adolescents and young adults with lifestyle-related behavioral exposures. While a limited number used longitudinal or prospective cohort designs. Most studies were cross-sectional. Previous systematic reviews have similarly demonstrated that sedentary behavior and prolonged screen exposure are consistently associated with obesity and cardiometabolic dysfunction in children and adolescents (15, 16). Sample sizes ranged from 95 college-aged adults in the United States to 58,712 children and adolescents in China (8, 25). Notably, most participants didn’t have severe chronic comorbidities; the observed associations are more likely to reflect true relationships rather than being influenced by confounding factors.
In terms of outcome measures, higher screen time and prolonged sedentary behavior were significantly associated with a high risk of obesity and metabolic disorders. Cheng et al. (14) reported that screen time over 3 hours per day was associated with an elevated risk of abdominal obesity and metabolic syndrome. In contrast, high sedentary time was also associated with elevated triglyceride levels and lower HDL-C levels. Similarly, Khan et al. (17) demonstrated that each additional hour of screen exposure increased the likelihood of metabolic syndrome among adolescents by 21%. Results were supported by Vella et al. (3), who reported that higher leisure screen time was independently associated with higher BMI, waist circumference, and fat mass, as well as higher triglycerides and lower cardiorespiratory fitness among college-aged adults. Similarly, Fernanda Rocha de Faria et al. (23) demonstrated that screen time for over 4 hours per day significantly increased the likelihood of belonging to a high-cardiometabolic-risk group. This can be attributed to reduced energy expenditure, unhealthy dietary behaviors, and prolonged sitting time. Of greater concern, sedentary behavior has recently been reported as an independent risk factor for insulin resistance and cardiometabolic dysfunction, even after adjustment for physical activity levels. In contrast, Al-Shoaibi et al. (24) reported no statistically significant association between screen time and transition from overweight or obesity to normal BMI. Such inconsistent findings may arise from variations in sample size, study setting, and design.
Sleep duration emerged as one of the most important protective factors against obesity and metabolic abnormalities in the included studies. Kurube et al. (2023) demonstrated strong inverse correlations between sleep duration and insulin resistance as well as fasting insulin levels among obese adolescents with metabolic syndrome in Indonesia (22). Moreover, Sehn et al. (2024) observed that higher baseline screen time predicted shorter sleep duration at follow-up, whereas higher BMI z-scores were associated with greater cardiometabolic clustering over time (12). In a prospective cohort study, Al-Shoaibi et al. (2026) reported that adolescents sleeping 9–11 hours/day were significantly more likely to transition from overweight or obesity to normal BMI percentile than those sleeping fewer hours (14). Smartphone-related sleep disruption was also highlighted by Alexander et al. (2025), who found that late-night smartphone use was associated with reduced sleep duration, delayed sleep onset, increased sedentary behavior, and lower daily step counts among adolescents from the ABCD cohort (18). Similarly, Riyas Basheer et al. (2025) reported significant associations among smartphone-using young adults between smartphone addiction, poorer sleep quality, increased BMI, and elevated blood pressure (19). These findings are biologically plausible because sleep deprivation alters leptin and ghrelin secretion, increases cortisol levels, impairs insulin sensitivity, and promotes dysregulated glucose metabolism (19, 20). Spiegel et al. demonstrated that sleep restriction reduces leptin levels while increasing ghrelin concentrations, thereby increasing appetite and caloric intake (26). In addition, Knutson reported that chronic sleep deprivation contributes to insulin resistance and increased cardiometabolic risk through neuroendocrine and inflammatory mechanisms (27).
Physical activity demonstrated a generally protective effect against obesity and cardiometabolic dysfunction across the included studies. Alkatan et al. (2021) found that higher physical activity among Kuwaiti college students was associated with lower body fat percentage and obesity, while lower screen time was inversely associated with higher activity levels (20). Similarly, Pitanga et al. (2019) demonstrated that physically active Brazilian adolescent boys with shorter screen time had significantly lower odds of being overweight compared with adolescents reporting low physical activity and prolonged screen exposure (16). Moitra et al (2021) further highlighted the combined effect of unhealthy behaviors, reporting that clustering of low physical activity, excess screen time, and poor sleep quality substantially increased obesity and central adiposity risk, particularly among girls (13). These findings are supported by prior evidence that regular moderate-to-vigorous physical activity improves insulin sensitivity, lipid metabolism, and energy balance, while reducing adiposity and cardiometabolic risk (28). Ekelund et al. showed that increased physical activity attenuates the harmful metabolic effects of sedentary behavior among adolescents and young adults (28). Similarly, Janssen and LeBlanc concluded that regular physical activity significantly improves cardiovascular and metabolic health indicators in school-aged populations (29). Therefore, the interaction among physical inactivity, excessive screen exposure, and sleep disruption likely contributes synergistically to the development of obesity rather than acting through isolated pathways alone.
Quality Assessment
Most studies demonstrated good methodological quality according to the Newcastle–Ottawa Scale, particularly the cohort studies conducted by Sehn et al. (1), Alexander et al. (8), and Al-Shoaibi et al. (14). Moreover, several cross-sectional studies demonstrated robust sampling methods and comprehensive cardiometabolic assessments. Nevertheless, moderate-quality studies were limited by smaller sample sizes, reliance on self-reported behavioral measures, and limited adjustment for confounding variables. Thus, residual confounding and recall bias may have influenced some reported associations. However, the consistency of findings across studies with varying methodologies strengthens confidence in the conclusion that excessive screen time, sedentary behavior, and sleep disruption contribute significantly to obesity and metabolic syndrome among adolescents and young adults.
Limitations
This systematic review is limited by the predominance of cross-sectional studies, which restricts causal inference and limits assessment of relationships between behavioral exposures and cardiometabolic outcomes. It is further limited by considerable heterogeneity regarding exposure definitions, sleep duration thresholds, and cardiometabolic outcome assessment. Additionally, many studies relied on self-reported questionnaires, thereby increasing the risk of recall and reporting bias. Future research should focus on large-scale longitudinal and interventional studies that use standardized protocols and objective behavioral monitoring tools.
Conclusion
Given the growing burden of obesity and metabolic syndrome globally, Modifiable lifestyle-related habits such as excessive screen time, sedentary behavior, and inadequate sleep duration are associated with adverse obesity and cardiometabolic outcomes among adolescents and young adults. Given the growing burden of obesity and metabolic syndrome globally, reducing recreational screen exposure, improving sleep hygiene, and promoting regular physical activity should represent important public health priorities. Importantly, future large-scale studies with standardized methodologies are needed to assess the interaction between lifestyle behaviors and metabolic risk accurately and to identify individuals at risk.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding.
Ethical consideration
No considerations.
Data availability
All data is available within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.