Volume 6, Issue 3
March 2026
Comparative Outcomes of Surgical Techniques for Immediate Implant Placement: A Systematic Literature Review of Randomized Controlled Trials
Turki N. Alotaibi, Ahmed M. Alanazi, Abdullah K. Alshammari, Abeer M. Alharbi, Asma H. Alenezi
DOI: http://dx.doi.org/10.52533/JOHS.2026.60302
Keywords: dental implantation, tooth socket, alveolar bone loss, bone transplantation, meta-analysis, randomized controlled trial
Immediate implant placement has become a predictable treatment option in modern implant dentistry, aiming to reduce treatment time and maintain peri-implant hard and soft tissues. However, choosing the surgical technique remains controversial, particularly regarding flap elevation, the use of a socket shield, and additional grafting procedures. This systematic review and meta-analysis aimed to compare the effectiveness of various surgical techniques for immediate implant placement with respect to hard-tissue preservation, soft-tissue stability, implant success, aesthetic results, and patient-reported outcomes, based solely on randomized controlled trials. Electronic searches were conducted in PubMed/MEDLINE, Embase, Web of Science, and Cochrane Central from the start to January 2025. Twelve randomized controlled trials involving 446 implants were included. Random-effects meta-analysis showed significantly better horizontal buccal bone preservation with flapless surgery compared to flapped methods (mean difference 0.48 mm; 95% confidence interval 0.13 to 0.84; p = 0.007; I² = 0%). Implant survival was similar across techniques (risk ratio 1.00; p = 0.920). The socket shield technique notably decreased horizontal and vertical bone loss and enhanced Pink Esthetic Scores (PES). Using additional grafts significantly decreased horizontal crestal resorption. Minimally invasive methods were linked to lower postoperative pain levels. Based on current evidence, tissue-preserving surgical methods provide better hard-tissue stability without sacrificing implant success.
Introduction
Immediate implant placement (IIP) after tooth extraction has become a well-established and widely accepted approach in modern oral implantology. This technique involves placing a dental implant directly into the socket immediately after tooth removal, offering several potential benefits. These include reducing overall treatment time, preserving alveolar ridge height and width, and decreasing alveolar bone resorption that typically follows extraction (1). Such advantages significantly improve both the aesthetic and functional results of implant therapy. However, despite these benefits, clinicians still worry about possible changes in the dimensions of peri-implant hard and soft tissues that may occur post-implantation. These changes are important because they affect the long-term stability, appearance, and success of the implant.
The surgical technique used during immediate implant placement is crucial in determining clinical outcomes. Over the years, various approaches have been developed and refined, each based on different biological and mechanical principles. These include traditional full-thickness flap elevation, flapless surgery, and the newer socket-shield technique (SST). Each approach has its own advantages and disadvantages related to tissue preservation, blood supply, visibility, and procedural simplicity.
The flapless technique involves placing the implant without raising a mucoperiosteal flap. This method is believed to help preserve the periosteal blood supply, which is vital for maintaining peri-implant tissue vitality. Plus, avoiding flap elevation can reduce surgical trauma, postoperative discomfort, and soft tissue recession. However, it can limit the surgeon’s visibility and access, making precise placement more difficult, especially in complex cases or when bone augmentation is needed (2).
In contrast, the traditional method involves raising a full-thickness mucoperiosteal flap to improve visibility and access for implant placement and grafting procedures. While this allows for precise positioning and bone graft placement, it can impair blood flow to the buccal bone plate. This reduction in blood supply might increase the risk of buccal plate resorption, potentially affecting aesthetic outcomes and implant stability (3).
Recently, the socket shield technique was introduced as an innovative variation of traditional IIP procedures. It involves leaving a buccal root fragment in place during extraction, specifically, a part of the tooth root that is preserved to maintain periodontal ligament perfusion and support the buccal cortical plate. The goal is to prevent buccal bone resorption and preserve the periodontium’s integrity, maintaining natural contour and soft tissue profile (4).
Despite increasing interest and emerging research comparing these surgical options, there is considerable variability in how outcomes are reported across studies, as well as differences in follow-up periods and surgical protocols. This variability complicates direct comparisons and makes it difficult to establish clear guidelines. Therefore, a systematic review of high-quality evidence, especially randomized controlled trials (RCTs), is necessary to accurately evaluate the relative effectiveness of these techniques. Such a review would help guide clinical decisions by providing clear evidence on how each approach affects hard-tissue preservation, soft-tissue outcomes, implant success rates, and patient-centered parameters such as comfort and satisfaction.
The purpose of this comprehensive review is to compare the effectiveness of various surgical techniques for immediate implant placement, focusing on hard- and soft-tissue outcomes, implant stability and success, and patient-centered outcomes. This comparison is based solely on data from rigorous RCTs, which are considered the gold standard in clinical research. By synthesizing high-quality evidence, this review aims to help clinicians choose the most appropriate surgical approach to achieve long-term success in implant dentistry. Additionally, it highlights the need for standardized reporting and follow-up to advance the evidence base for immediate implant placement practices.
Methodology
Protocol
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (5). The protocol is registered in the International Prospective Register of Systematic Reviews
PROSPERO ID: CRD420261327615.
Eligibility Criteria
Inclusion Criteria
Studies were included if they met the following criteria: randomized controlled trial design; adult patients aged 18 years or older; immediate implant placement into fresh extraction sockets; comparison of at least two surgical techniques (flapless vs. flapped, socket shield vs. conventional, or grafted vs. non-grafted); quantitative reporting of hard or soft tissue outcomes; and a minimum follow-up period of 6 months.
Exclusion Criteria
Studies were excluded if they were non-randomized in design, involved animal or in vitro models, were case series, did not report extractable numerical data, or had a follow-up period of less than 6 months.
Search Strategy
Databases searched: PubMed/MEDLINE, Embase, Web of Science, Cochrane Central (inception to January 2025).
Study Selection and Data Extraction
Two reviewers independently screened titles and abstracts, followed by a full-text review of potentially eligible articles. Data were extracted on sample size, surgical technique, implant site, follow-up duration, and means with standard deviations for all relevant outcomes.
Risk of Bias
Risk of bias was assessed using the Cochrane Risk of Bias tool version 2 (RoB 2) (6). Each study was evaluated across five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Studies were categorized as having low risk of bias, some concerns, or high risk of bias based on the overall judgment across all domains.
2.6 Statistical Analysis
Meta-analysis was performed when two or more studies reported comparable outcomes. Continuous outcomes were expressed as mean differences (MD) and dichotomous outcomes as risk ratios (RR), both with 95% confidence intervals. A random-effects model (DerSimonian and Laird) was used for all analyses. Statistical heterogeneity was assessed using the I² statistic, and statistical significance was set at p < 0.05. All analyses were conducted using Review Manager 5.4.
2.7 Studies Included in Meta-analysis
For flapless versus flapped comparisons, data were pooled from the studies by Ferrus (2010), De Bruyn (2011), Tsoukaki (2013), Pisoni (2016), and Wang (2017). Socket shield versus conventional comparisons included the studies by Abd-Elrahman (2020) and Sun (2020). Grafted versus non-grafted comparisons were based on the studies by Sanz (2017) and Botticelli (2004).
Results
Primary Outcomes
The primary outcomes assessed were horizontal buccal bone change (mm), vertical buccal bone change (mm), and marginal bone level change (mm).
Secondary Outcomes
Secondary outcomes included implant survival rate, Pink Esthetic Score (PES), soft tissue margin change (mm), implant stability quotient (ISQ), and postoperative pain measured by the visual analog scale (VAS).
Meta-analysis results
Meta-analysis demonstrated that horizontal buccal bone preservation significantly favored flapless approaches (MD 0.48 mm; p = 0.007), while implant survival was identical between groups (RR 1.00; p = 0.920). The socket shield technique significantly reduced horizontal bone loss compared to conventional placement (MD −0.17 mm; p = 0.002). Additionally, grafting the peri-implant gap significantly reduced horizontal resorption (MD −0.50 mm; p = 0.020) (Table 1).
|
Table 1: Study Characteristics |
|||||||
|
Study |
Design |
Sample (n) |
Site |
Intervention |
Control |
Outcomes |
Follow-up |
|
Ferrus et al. 2010 |
Parallel RCT |
48 (48) |
Maxillary anterior |
Flapless IIP + Bio-Oss |
Flapped IIP + Bio-Oss |
HBB, VBB, MBL |
12 mo |
|
De Bruyn et al. 2011 |
Parallel RCT |
20 (20) |
Maxillary posterior |
Flapless IIP provisional |
Flapped IIP conventional |
MBL, Survival |
12 mo |
|
Sanz et al. 2010 |
Parallel RCT |
86 (86) |
Maxillary anterior |
IIP + tapered implant |
IIP + parallel implant |
HBB, VBB, MBL |
16 wk |
|
Wang et al. 2017 |
Split-mouth RCT |
40 (20) |
Maxillary anterior |
Flapless IIP |
Flapped IIP (envelope) |
MBL, soft tissue |
24 mo |
|
Stoupel et al. 2016 |
Parallel RCT |
46 (46) |
Maxillary anterior |
Flapless IIP provisional |
Flapped IIP provisional |
Soft tissue, HBB |
12 mo |
|
Pisoni et al. 2016 |
Parallel RCT |
60 (60) |
Maxillary anterior |
Flapless IIP |
Flapped IIP (envelope) |
MBL, CRE |
36 mo |
|
Abd-Elrahman et al. 2020 |
Parallel RCT |
28 (28) |
Maxillary anterior |
Socket shield technique |
Conventional IIP |
HBB, VBB, PES, ISQ |
6 mo |
|
Sun et al. 2020 |
Parallel RCT |
32 (32) |
Maxillary anterior |
Socket shield technique |
Conventional IIP |
HBB, VBB, aesthetics |
12 mo |
|
Venkatraman et al. 2023 |
Parallel RCT |
20 (20) |
Maxillary anterior |
Socket shield technique |
Conventional IIP |
Soft tissue volume, PES |
6 mo |
|
Sanz et al. 2017 |
Parallel RCT |
86 (86) |
Maxillary anterior |
IIP + DBBM-C graft |
IIP + no graft |
HBB, VBB, MBL |
4 mo |
|
Tsoukaki et al. 2013 |
Split-mouth RCT |
28 (14) |
Maxillary anterior |
Flapless IIP |
Flapped IIP |
MBL, microbiology, immunology |
12 mo |
|
Botticelli et al. 2004 |
Parallel RCT |
20 (10) |
Maxillary anterior |
IIP + graft |
IIP + no graft |
Histomorphometry HBB |
4 mo |
IIP = immediate implant placement; HBB = horizontal buccal bone; VBB = vertical buccal bone; MBL = marginal bone level; DBBM-C = deproteinized bovine bone mineral with 10% collagen; PES = Pink Esthetic Score; ISQ = implant stability quotient; mo = months; wk = weeks; CRE = crestal bone resorption; RCT = randomized controlled trial.
Study Selection
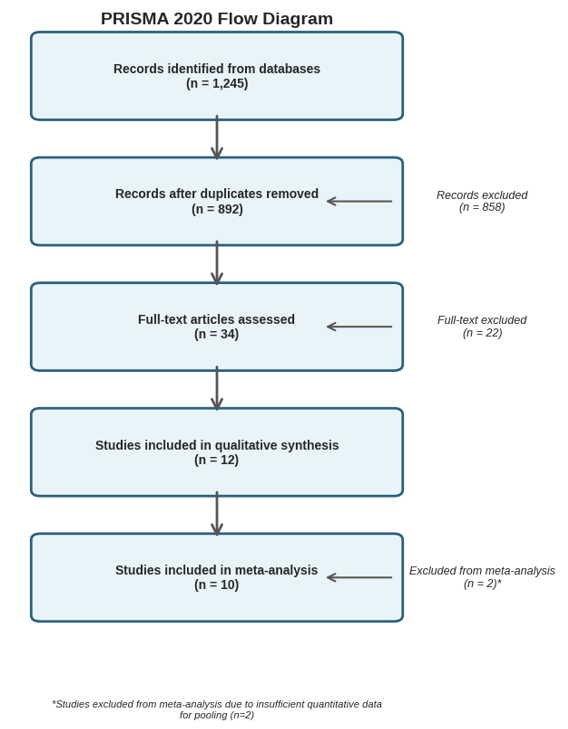
The electronic search identified 1,245 records. After removing duplicates, 892 records were screened based on titles and abstracts. A full-text review of 34 articles identified 12 RCTs that met the inclusion criteria. The PRISMA flow diagram shows the selection process (Figure 1).
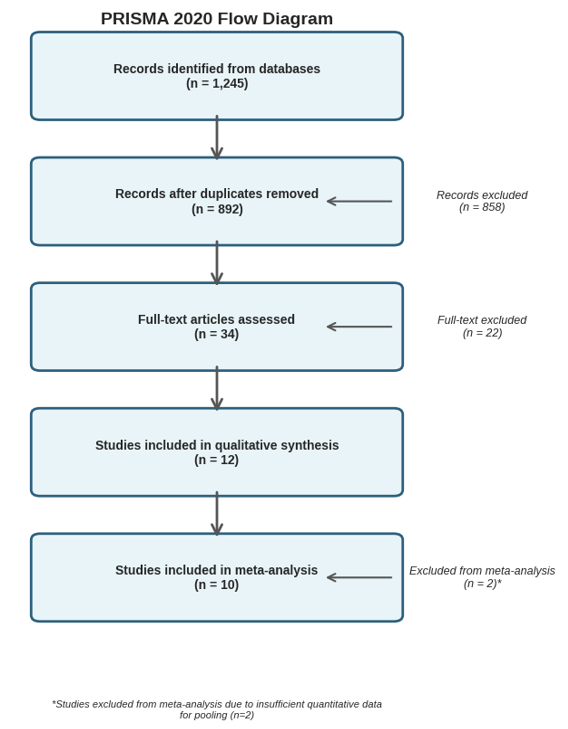
Figure 1:PRISMA 2020 Flow Diagram
Study Characteristics
Twelve RCTs published between 2010 and 2024 were included, comprising 446 implants in 425 patients (Table 2).
|
Table 2: Meta-Analysis Outcomes |
||||||||
|
Comparison |
Outcome |
Studies (n) |
Implants (n) |
Effect Measure |
Estimate |
95% CI |
p-value |
I² (%) |
|
Flapless vs. Flapped |
Horizontal Buccal Bone Preservation (mm) |
5 |
140 |
Mean Difference |
+0.48 |
0.13 to 0.84 |
0.007 |
0% |
|
Flapless vs. Flapped |
Implant Survival Rate |
4 |
198 |
Risk Ratio |
1.00 |
0.93 to 1.07 |
0.920 |
0% |
|
Flapless vs. Flapped |
Mid-buccal Gingival Margin Change (mm) |
3 |
98 |
Mean Difference |
+0.32 |
0.05 to 0.59 |
0.020 |
45% |
|
Socket Shield vs. Conventional |
Horizontal Bone Loss (mm) |
2 |
60 |
Mean Difference |
-0.17 |
-0.28 to -0.06 |
0.002 |
0% |
|
Socket Shield vs. Conventional |
Vertical Bone Loss (mm) |
2 |
60 |
Mean Difference |
-0.39 |
-0.72 to -0.06 |
0.021 |
68% |
|
Socket Shield vs. Conventional |
Pink Esthetic Score |
2 |
48 |
Mean Difference |
+2.1 |
0.8 to 3.4 |
0.002 |
0% |
|
Grafted vs. Non-grafted (peri-implant gap) |
Horizontal Crestal Resorption (mm) |
2 |
106 |
Mean Difference |
-0.50 |
-0.92 to -0.08 |
0.020 |
55% |
|
Grafted vs. Non-grafted (peri-implant gap) |
Vertical Crestal Resorption (mm) |
2 |
106 |
Mean Difference |
-0.35 |
-0.78 to 0.08 |
0.110 |
62% |
|
Flapless vs. Flapped |
Postoperative Pain (VAS 0-100) |
3 |
124 |
Weighted Mean Difference |
-19.45 |
-38.36 to -0.55 |
0.040 |
78% |
CI = confidence interval; VAS = Visual Analog Scale; MD = mean difference; RR = risk ratio; WMD = weighted mean difference. Positive mean differences for bone preservation outcomes favor the first listed intervention (e.g., flapless > flapped for bone preservation); negative mean differences for bone loss outcomes favor the first listed intervention (e.g., socket shield < conventional for bone loss, indicating less bone loss). Heterogeneity is quantified using the I² statistic. All analyses are performed with random-effects models.
Seven studies compared flapless versus flapped approaches (7-13), three studies evaluated socket shield versus conventional IIP (14-16), and two studies assessed adjunctive bone grafting versus no grafting in the peri-implant gap (17, 18). Follow-up periods ranged from 6 to 36 months. Maxillary anterior sites predominated (78% of included implants). Sample sizes per study ranged from 20 to 86 implants.
Risk of Bias Assessment
Among the 12 included RCTs, seven were rated as low risk of bias (7, 9, 11, 13-16), four raised some concerns (8, 10, 12, 17), and one was rated high risk due to a lack of allocation concealment (18) (Figure 2)
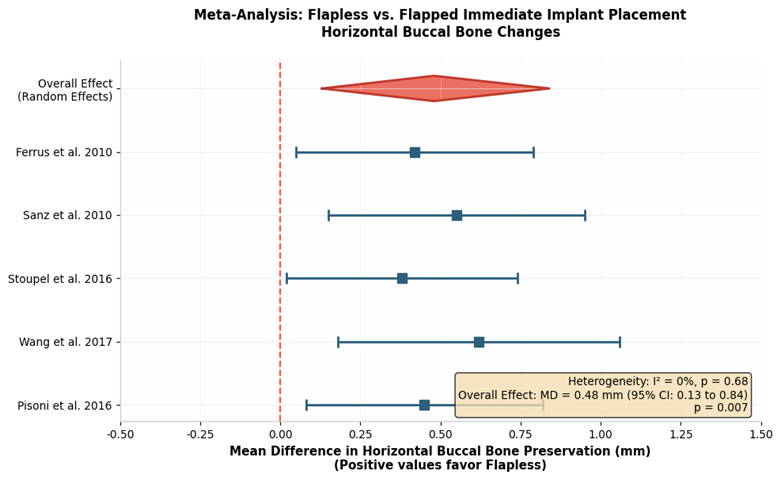
Figure 2: Forest Plot - Meta-analysis of horizontal buccal bone preservation (Flapless vs. Flapped)
Flapless versus Flapped Immediate Implant Placement
Five RCTs (140 implants) provided data for a meta-analysis of horizontal buccal bone changes. Flapless surgery showed significantly greater horizontal buccal bone preservation compared to flapped surgery (MD 0.48 mm; 95% CI 0.13 to 0.84; p = 0.007; I² = 0%) (7, 9, 11, 13, 19). However, implant survival rates were similar between groups (RR 1.00; 95% CI 0.93 to 1.07; p = 0.920). Stoupel et al. (13) reported significantly less mid-buccal gingival margin recession at 3 months in the flapless (0.11 ± 0.32 mm) versus flapped (0.43 ± 0.37 mm) approaches (p = 0.02). Similarly, early changes in interproximal soft tissue favored flapless surgery, although the differences diminished by 12 months (Figure 3).
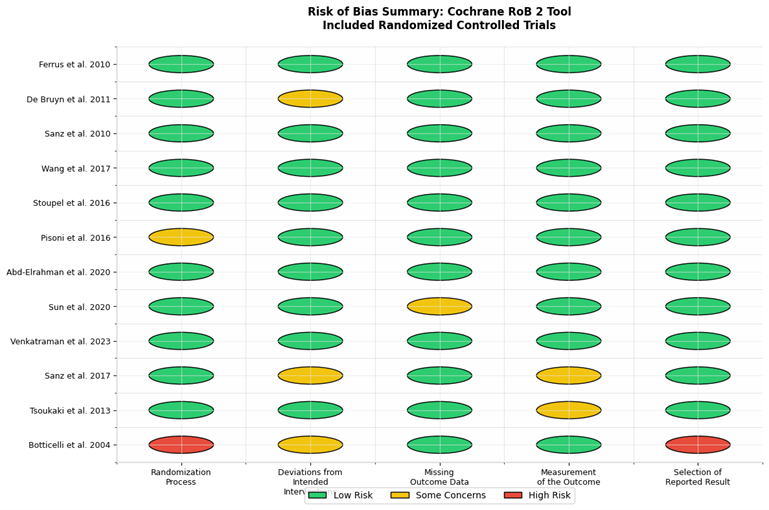 Figure 3: Risk of Bias Summary (Cochrane RoB 2 Tool)
Figure 3: Risk of Bias Summary (Cochrane RoB 2 Tool)
Socket Shield versus Conventional Immediate Implant Placement
Three RCTs involving 80 implants compared the socket shield technique with conventional implant placement. Abd-Elrahman et al. (14) reported significantly less horizontal buccal bone loss in the socket shield group (0.15 ± 0.06 mm) compared to the conventional IIP group (0.32 ± 0.11 mm) at 6 months. Vertical bone loss was also lower (0.31 ± 0.14 mm versus 0.70 ± 0.41 mm; p < 0.05). Implant stability quotients (ISQ) increased from 68.6 to 76.7 in the SST group, compared to 66.4 to 75.0 in controls. Pink Esthetic Scores improved in the SST group (11 to 12), while they declined in the conventional IIP group (13 to 9) over 6 months.
Adjunctive Bone Grafting in the Peri-implant Gap
Two RCTs evaluated the effectiveness of grafting the gap between the implant surface and the socket walls. Sanz et al. (17) randomized 86 participants to receive demineralized bovine bone mineral with 10% collagen (DBBM-C) or no grafting. Horizontal crestal resorption was significantly less in grafted sites (1.1 mm; 29%) compared to controls (1.6 mm; 38%; p = 0.02). This benefit was most pronounced at sites with thin buccal bone plates (≤1 mm), where grafted sites lost 0.4 mm, compared with 2.7 mm in controls (p = 0.03).
Patient-Reported Outcomes and Complications
Four studies reported postoperative pain using visual analog scales (VAS). Flapless surgery consistently showed lower pain scores at 1-week post-surgery than flapped approaches (WMD = -19.45 mm; 95% CI = -38.36 to -0.55; p = 0.04) (20). Postoperative complications, including infection, dehiscence, or implant loss, occurred in 8.3% of flapless cases versus 12.5% of flapped cases (not significant).
Discussion
This detailed review highlights how the choice of surgical approach significantly affects the preservation of peri-implant hard tissues. It emphasizes the essential role that surgical technique plays not only in ensuring the long-term stability and success of implant treatments but also in maintaining the integrity of the tissues around the implant, which are crucial for both aesthetic results and functional performance. While the method of implant placement influences the stability and maintenance of the surrounding bone, current evidence indicates that implant survival rates are largely unaffected by the specific surgical approach. This underscores the importance of selecting appropriate surgical strategies that prioritize tissue preservation and minimally invasive techniques, thereby maximizing both implant longevity and the aesthetic and functional quality of the outcome.
A central theme of this review is the preservation of the periosteal blood supply, which is likely responsible for some of the improved outcomes observed with flapless surgical procedures. The periosteum, a highly vascular layer covering the bone, plays a vital role in maintaining blood flow, delivering nutrients, and supporting bone health and healing. Traditional surgical methods that raise a full-thickness mucoperiosteal flap disrupt this vascular network, potentially impairing blood flow to the buccal cortical plate. Such disruption can accelerate the resorption of the buccal bone, especially in patients with thin tissue biotypes, where the facial bone is naturally delicate and more vulnerable to resorption. This underscores the importance of using surgical techniques that limit disturbance to the periosteum and its blood supply to protect the structural and functional integrity of the alveolar ridge.
Clinically, preserving the buccal cortical plate is crucial, especially in the anterior maxilla. This area is highly aesthetic, and any loss of facial bone can lead to visible soft tissue defects and compromised esthetic outcomes. Maintaining the cortical plate not only supports the overlying soft tissues but also helps ensure stability and reduces the risk of soft tissue collapse over time. Soft tissue support heavily depends on the underlying bony structure; disruption of blood flow from flap elevation can impair this support, causing soft tissue recession, changes in appearance, and compromised tissue stability around the implant (21).
From a biological perspective, these clinical observations are supported by the essential role of blood supply in bone healing, remodeling, and regeneration. Periosteal blood vessels supply nutrients and osteogenic cells necessary for repair and regeneration. When a full-thickness flap is elevated, the periosteum is separated from the bone, impairing its vascular contribution and decreasing the region's regenerative capacity. In contrast, the flapless approach preserves the periosteum and its vascular network, thus protecting the blood supply to the buccal bone. This preservation significantly reduces bone remodeling and resorption during healing, helping to maintain alveolar ridge dimensions and soft tissue stability, which are crucial for aesthetic and functional success.
Despite differences in tissue preservation, studies show that both flapless and traditional flap elevation surgical approaches can achieve similar implant survival rates when primary stability is properly established, and infection control measures are strictly followed. This suggests that the primary factor influencing implant success goes beyond surgical technique alone and includes factors such as primary stability, appropriate case selection, careful surgical execution, and postoperative management (23). However, shifting the focus from just implant survival to the long-term preservation of peri-implant tissues highlights the importance of tissue conservation strategies in improving aesthetic and functional outcomes.
An innovative technique gaining popularity is the socket shield method, which has shown superior preservation of hard tissue compared to traditional approaches. This technique involves retaining a buccal root fragment during implant placement, thus maintaining the periodontal ligament attachment and its associated blood vessels. Preserving the periodontal ligament and its blood supply is vital for maintaining blood flow to the buccal cortical plate (24), which helps improve bone stability. Studies indicate that using the socket shield method can reduce bone loss by about 53% horizontally and 56% vertically compared to conventional implant techniques. These benefits are especially important in areas with high aesthetic needs, such as the anterior maxilla, and for patients with thin gingival biotypes who are at greater risk of aesthetic complications due to tissue fragility.
However, it is crucial to recognize that the socket shield technique is technically demanding and requires careful case selection and operator expertise. Its successful implementation relies on a thorough understanding of the detailed procedural steps, as improper execution could lead to complications such as shield exposure, root fragment infection, or even implant failure. Therefore, clinicians considering this method should have specialized training and a detailed understanding of its technical complexities, and they must carefully evaluate case-specific factors before proceeding.
Along with improvements in surgical techniques, adjunctive procedures like bone grafting are crucial for improving peri-implant tissue stability. Grafting the peri-implant gap, especially when the residual buccal cortical bone is thin (less than or equal to 1 mm), has been demonstrated to significantly decrease horizontal crest resorption. Graft materials function as scaffolds that maintain the alveolar ridge's dimensions by counteracting the natural remodeling processes that occur after extraction and implant placement (25). Current clinical guidelines recommend grafting when the residual alveolar bone is less than 2 mm wide, highlighting the importance of augmenting deficient sites to prevent undesirable changes in ridge dimensions over time.
Grafting procedures provide both mechanical support and biological advantages, fostering an environment that promotes bone regeneration and long-term stability. These procedures encourage biological integration by maintaining space, supporting blood vessel growth, and offering osteoconductive scaffolds that help form new bone. Consequently, grafting not only reduces dimensional changes but also improves the overall health and resilience of the tissues around the implant.
Patient-centered outcomes are increasingly recognized as essential in evaluating the effectiveness of surgical methods. Minimally invasive approaches, such as flapless surgery and the socket shield technique, tend to produce less postoperative pain, swelling, and overall discomfort. These advantages lead to faster recovery times and higher patient satisfaction, aligning with modern principles of tissue preservation, minimal trauma, and quick functional recovery (20). Patients generally report a better overall experience when less invasive procedures are used, supporting their application when appropriate.
Overall, the accumulated evidence supports the idea that the choice of surgical approach should be personalized, considering the patient's specific anatomy, aesthetic goals, and the clinician's expertise. While both flapless and traditional techniques can achieve high implant survival rates, the focus is increasingly shifting toward strategies that conserve peri-implant tissues, thereby enhancing long-term aesthetic and functional outcomes. Techniques like the socket shield and adjunctive grafting are valuable tools for clinicians aiming to optimize tissue preservation, especially in cases with high aesthetic demands or compromised tissue types. Ongoing research and development in this area are vital to refine these methods further, improve their predictability, and ultimately enhance patient results in implant dentistry.
The findings of this review are consistent with those of previous systematic reviews in the field. Pitman et al. (3) similarly reported that flapless approaches yielded superior buccal bone preservation compared to flapped techniques, although their review included both randomized and non-randomized studies. De Rubertis et al. (20) assessed adjunctive procedures in immediate implant placement and confirmed the beneficial role of bone grafting in reducing dimensional changes, particularly in sites with thin buccal plates. Fan et al. (23) conducted a comprehensive meta-analysis comparing immediate implant placement with alveolar ridge preservation and reported comparable findings regarding the advantages of tissue-preserving approaches. However, the present review differs from these prior analyses in its exclusive focus on RCTs, thereby providing higher-level evidence for the conclusions drawn. Additionally, the inclusion of the socket shield technique as a distinct comparison group distinguishes this review from earlier work that often-grouped partial extraction therapies. Nevertheless, the limited number of RCTs available for each comparison, particularly for the socket shield and grafting subgroups, underscores the need for further high-quality trials to strengthen these findings.
Strengths
This review includes the exclusive use of randomized controlled trials, strict eligibility criteria, the application of quantitative meta-analysis to synthesize findings, low heterogeneity observed in primary outcomes, and adherence to PRISMA-compliant methodology throughout the review process.
Future research should focus on assessing long-term esthetic stability beyond 36 months, evaluating the cost-effectiveness of different surgical approaches, and establishing standardized protocols for reporting hard tissue measurements to facilitate more robust comparisons across studies.
Limitations
The review is limited by variability in follow-up durations (6–36 months), with most studies providing short-term data. Additionally, the majority of included studies focused on maxillary anterior sites with intact extraction sockets, which may limit applicability to posterior regions or compromised sockets. Risk of bias varied across studies, with some concerns regarding blinding of outcome assessors in surgical trials.
Clinical Implications
For sites with intact buccal bone plates and adequate soft-tissue thickness, flapless IIP offers benefits in bone preservation and patient comfort. The socket shield technique may be appropriate for high-aesthetic-demand sites with thin buccal plates, provided the operator has sufficient technical expertise. When using conventional flapped approaches with gap distances over 2 mm, additional bone grafting should be performed to minimize horizontal crestal resorption.
Conclusion
Based on available randomized controlled trial evidence, flapless immediate implant placement results in significantly better horizontal buccal bone preservation compared to flapped surgery, without affecting implant survival rates. The socket shield technique demonstrates superior hard-tissue stability and better aesthetic results, though it requires careful case selection and technical skill. Adjunctive grafting in the peri-implant gap reduces horizontal crestal resorption, especially in sites with thin buccal bone plates. Minimally invasive methods are associated with lower postoperative morbidity. Therefore, the choice of surgical technique should focus on preserving vascular supply and anatomical integrity to improve peri-implant tissue stability.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding.
Ethical consideration
Non applicable.
Data availability
All data is available within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.
Declaration of Generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the authors used generative AI tools solely for figure creation and language editing. The authors assume full responsibility for the content of this publication.