Volume 6, Issue 2
February 2026
Improving Patient Appointment Availability through Enhanced Telehealth Services
Jowharah Alosaimia, Turki Alharbi, Maha Bin Shafi, Bushra Alhakami, Nasser Alharthi, Muhammed Abdulmughaith, Azam Alotaibi, Nawaf Alaqeel, Muhammed Sulaiman, Buthainah Alshathri
DOI: http://dx.doi.org/10.52533/JOHS.2026.60203
Keywords: Women's Health, Timely Care, Patient Access, Telehealth Utilization, Patient Satisfaction, No-Show Rates, Virtual Assessments
Background: Access to timely care is a critical component of quality healthcare, particularly in women’s health services, where demand is consistently high. Delays in appointment scheduling and long wait times can compromise patient outcomes, reduce satisfaction, and strain healthcare resources. Addressing these challenges requires systemwide interventions aimed at optimizing patient flow, enhancing access to care, and promoting the use of alternative care modalities such as telehealth. In this project, we are testing the impact of targeted interventions on appointment wait times, patient throughput, telehealth utilization, patient satisfaction, and the no-show rates at a Women’s Health Clinic.
Local Problem: Extended periods for the next available appointments at the Women’s Health Clinics in Wazarat Primary Care Centre have reached up to 75 days, compromising women's access to essential healthcare and underscoring the need for effective intervention.
Methods: In the third quarter of 2024, the quality improvement project implemented virtual assessments for all late scheduled appointments at the Women’s Health Clinic in Wazarat Primary Care Centre, Prince Sultan Military Medical City. This involved conducting necessary tests, timely cancer screenings, and referring patients to follow-up services. Follow-up appointments were scheduled remotely to discuss results and monitor treatment, while in-person visits were reserved for cases requiring clinical examinations, such as Pap smears.
Interventions: In this project, we conducted virtual assessments via phone calls for all late-scheduled appointments. This approach prioritized around 900 patients who were waiting for in-person appointments, thus minimizing unnecessary visits. Comprehensive virtual follow-ups communicated diagnostic results, fostering ongoing therapeutic relationships and enhancing patient engagement.
Results: The intervention resulted in a 75% reduction in the third next available appointment time (from 75 days to 15) and an 85% decrease in the no-show rates. Also, patients’ satisfaction level was improved, demonstrating the success of the project.
Conclusions: This project established a responsive healthcare framework that promotes preventive care and optimizes resource allocation. Our innovative solutions tackle the unique challenges of improving appointment availability and serve as a model for integrating virtual care into traditional health systems, demonstrating our commitment to enhancing healthcare accessibility and quality for women.
Introduction
Our quality improvement project, initiated in the last weeks of Q3 2024, identified a concerning trend in women's health clinics in the Wazarat primary care center. The time from patient referral to the next third available appointment (The time to the next available appointment (TNAA)). has risen to an unacceptable average of 75 working days, exceeding the optimal target of less than 14 days. In addition, the no-show rate was up to 30% due to long waiting times or patient seeking care in the private health sector. This delay significantly hinders timely healthcare delivery, especially in preventive care and screening services for conditions like breast and cervical cancer. Prolonged waiting times in women's health clinics pose a systemic challenge that impacts essential healthcare services. Such delays compromise early detection and intervention, potentially leading to poorer health outcomes and increased morbidity (1).
Research has shown that extended wait times significantly decrease the rates of essential screenings for conditions such as breast, cervical cancer, and colorectal cancer (2). A study published on the barriers and facilitators of breast cancer screening among Saudi women showed that only 48.9% from a total of 476 participants had undergone breast cancer screening at least once in their lives (3). This gap underscores the urgent need for innovative solutions, such as telemedicine, which can facilitate quicker access to care and significantly reduce appointment delays.
Furthermore, the impact of telehealth services on patient satisfaction has been well documented (4-5). A review from the Agency for Healthcare Research and Quality revealed that women seeking preventive care expressed high satisfaction scores when utilizing telehealth services (6). The convenience of virtual consultations was particularly valued; it improves access to care as it minimizes travel time and increases compliance with screening recommendations (7).
Telehealth interventions could reduce the TNAA and the no-show rates for follow-up visits, as demonstrated in one study. The time until the new patient visit was 37 days for an in-person visit and 19 days for a video call visit, while no show rate was 3.3% for a remote follow-up visit and 11.1% for in person visit. (8) This evidence highlights telemedicine's effectiveness in addressing barriers to care, especially in underserved populations, leading to enhanced engagement and improved health outcomes.
Locally in Saudi Arabia, a study at a Saudi General Public Hospital in the Journal of King Saud University reported average utilization time for the clinics was only 30% of the allocated time in Riyadh, driven by a late physician arrival and early clock-out. (9) The introduction of telehealth services can be a viable strategy to improve access and improve efficiency and clinic time utilization. (10)
This project was informed by established public health models, including the Health Belief Model and the Donabedian Model of health care quality. This is further elaborated in the Methods section and provides a more comprehensive understanding of the intervention design and expected efficacy. Research indicates that delays in preventive screenings correlate with an increase in late-stage cancer diagnoses, complicating treatment and negatively affecting morbidity and mortality rates. Additionally, long waiting times can increase patient anxiety and deter individuals from seeking care, exacerbating health neglect and resulting in poor outcomes. Although breast cancer screening can reduce mortality, it also carries risks, particularly the potential for overdiagnosis, which may lead to unnecessary treatments and associated adverse effects.
It is essential to support women in making informed decisions about screening based on their individual values and preferences. Future challenges include improving the accuracy of estimates regarding the benefits and risks of screening, as well as gaining a deeper understanding of women’s values and preferences related to breast cancer screening. This gap emphasizes a critical deficiency in healthcare delivery that requires immediate attention.
Addressing this issue could enhance health outcomes, improve patient satisfaction, and reduce the economic burden of advanced disease treatment. By optimizing appointment availability, we can prioritize preventive care and facilitate timely interventions, ultimately improving women's overall health.
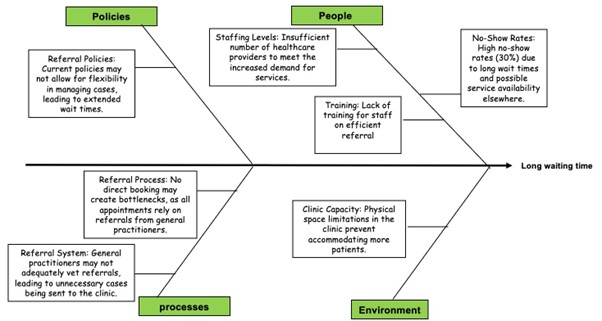
Improving timely access to well-woman care by reducing the TNAA for women’s health services from 75 days to 14 days through the implementation of telehealth services by the end of the 3rd quarter 2024. To meet these challenges, our project aims to implement a virtual clinic model that leverages telehealth solutions, focusing on the reasons presented in the following fishbone (Figure 1).
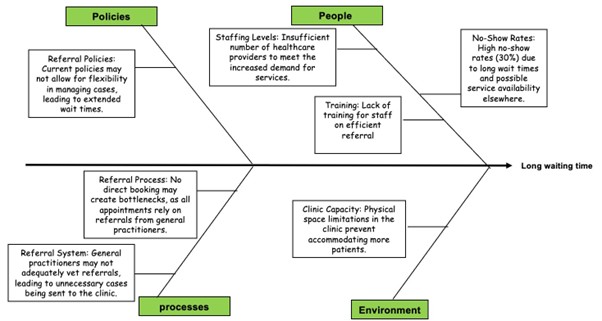
Figure 1: Fishbone for the reasons of long waiting time to access care
Methodology
Context
The Women’s Health Clinic, part of the Primary Care Department at Prince Sultan Military Medical City, provides specialized healthcare services exclusively for women. It operates in six centres out of a total of 17, offering comprehensive care for women of all age groups, focusing particularly on early screenings for cancers and osteoporosis based on age criteria. The clinic also addresses safe contraceptive methods, management of menopause related symptoms, and other women's health issues. Wazarat Centre is one of the largest primary care centres, providing services through four clinics each week and accommodating about 80 patients weekly, with a total of 320 patients per month. Due to its prominence and the increasing demand for services, the Wazarat Centre is experiencing significant pressure on appointment availability, leading to extended waiting times.
Access to these clinics is facilitated through referrals from general practitioners at primary care centres, as direct booking is not permitted. Despite ongoing efforts to raise awareness about the importance of early screening, there has been a marked increase in referrals to the clinics. Since the year 2023, demand for transfers to the Wazarat Centre has surged, resulting in waiting times extending beyond 15 weeks. This prolonged wait is particularly acute at the Wazarat Centre, as it is the largest facility and has seen a dramatic increase in patient demand. This situation not only delays service but also contributes to overcrowding in the waiting areas, negatively impacting the overall patient experience. Such crowding creates an uncomfortable environment and can discourage patients from seeking timely care. Additionally, the no-show rate for appointments has reached 30%, which is attributed to long waiting times and the availability of services elsewhere.
To address these challenges, several corrective measures have been implemented, such as activating a vetting system for referrals and gradually increasing patient capacity. A telehealth clinic has also been established to facilitate follow-up on results. However, despite these efforts, appointment times have not improved as anticipated.
In response, the idea for a quality improvement project emerged, focusing on conducting remote evaluations for all pending appointments. The project is scheduled to take place from mid-August to mid-September and includes plans for scheduling a virtual assessment clinic daily, accommodating more patients per clinic. Only patients requiring immediate appointments will be scheduled, while others will be directed to a telehealth follow-up clinic for non-urgent results
To effectively implement these changes, we assessed the preparedness and capability of the clinical workforce, including physicians and nursing staff, for a transition to telehealth. This involved creating a clear understanding of both the conceptual and practical aspects of telemedicine, the specific communication needs of patients in a remote setting, and the necessary technology-enabled tools for delivering quality care. Through these efforts, we aim to optimize appointment organization and utilize clinic resources effectively to provide timely and efficient care to patients.
Our project aligns with the Health Belief Model, which posits that individuals are more likely to engage in health-promoting behaviors if they perceive a significant threat to their health and believe that taking specific actions would reduce this threat. In the context of women’s health, the prolonged waiting times for preventive screenings represent a barrier to timely care, potentially leading to severe health consequences, such as late cancer diagnoses. By implementing a virtual assessment clinic, we sought to mitigate this barrier, thereby encouraging women to prioritize their health through timely screenings.
In addition, the Donabedian model of healthcare quality proposes that improving the structure through the introduction of virtual clinics will, in turn, optimize the process by reducing the time to the next available appointment and reducing the no-show rates, ultimately improving adherence to evidence-based recommended screenings.
Several key assumptions underpinned the development of our intervention. First, we assumed that the integration of telemedicine would reduce the time required for patients to receive care, thereby decreasing the number of days from the time the patient referred to the next third available appointment (The time to the next available appointment (TNAA)). This assumption was supported by existing research that highlighted the effectiveness of telehealth in improving access to services.
Second, we assumed that patients would respond positively to virtual consultations, given the convenience and flexibility they offer. Literature indicates that patients value the time and cost savings associated with telehealth, as well as the ability to receive care from the comfort of their homes. Development of our intervention was supported by existing literature, which suggests that reducing barriers to care through telehealth can lead to significant improvements in appointment availability and patient satisfaction. We assumed the no-show rate was due to long waiting time and the need for travel to reach the service. We expected the virtual clinic would eliminate travel and time burdens that are frequently reported as a cause for not seeking essential evidence-based preventive care, which will improve compliance and patient satisfaction.
Intervention
The implementation of the proposed interventions was carried out by a multidisciplinary team from the Women’s Health clinic at Al-Wazarat Health Centre, Prince Sultan Military Medical City. The team included a team leader, facilitators, quality assurance personnel, administrative personnel, and physicians. The administrative assistant helped by scheduling the telehealth consultations and patient recall, while the physicians provided the virtual assessments and contributed to streamlining the referrals. The project lead oversaw the development of communication protocols and framework assessment, ensuring smooth integration and monitoring of the intervention’s impact. The facilitator ensured seamless communication between team members and reported to the team leader.
Lastly, quality assurance personnel worked as consultants to ensure the quality standards are maintained through the implementation.
The proposed driver diagram was developed to enhance access to timely women’s health services and improve patient experience at the Women’s Health Clinic in Wazarat Primary Care Centre (Figure 2). For this project, several strategies were implemented. We facilitated telehealth consultations by successfully scheduling and conducting 900 virtual clinic assessments for eligible patients within the one-month project duration, thereby improving patient accessibility and convenience. To reduce the no-show rate, by recall patients 3 times separately.
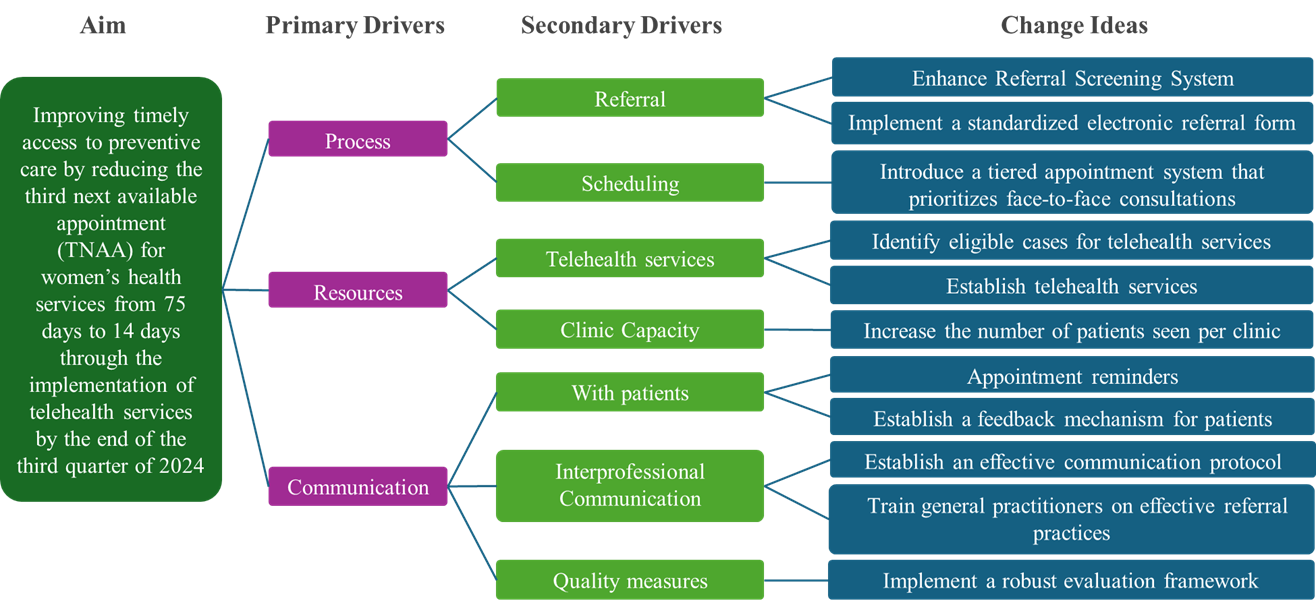
Figure 2: Driver diagram for change ideas to reduce TNAA
Additionally, we streamlined the referral process by prioritizing cases for Pap smears or vaginal examinations through a standardized electronic referral form and training general practitioners on effective referral practices to minimize unnecessary referrals. An efficient communication protocol was established between staff to optimize patient flow, care coordination, and follow-up processes throughout the project timeline.
To reduce wait times, we increased the number of patients seen per clinic session from 20 to 35-40 daily, with an average consultation time of 7-8 minutes. We also optimized scheduling by introducing a tiered appointment system that prioritizes face-to-face consultations while scheduling all other cases for telehealth follow-ups.
To measure quality outcomes, we implemented a robust evaluation framework to analyse patient feedback, appointment adherence, and clinical outcomes at the conclusion of the project. This data-driven approach helped refine the virtual clinic model and inform future quality improvement initiatives. We monitored the effectiveness of interventions and made data-driven adjustments by establishing a feedback mechanism for patients to share their experiences regarding time to appointment and service quality. This data was essential for refining processes and enhancing patient satisfaction.
Study of the intervention
The rationale for our project aimed at improving women's health services through virtual care and appointment availability is grounded in a formal framework that incorporates established models, concepts, and theories relevant to healthcare delivery and quality improvement. We employed the Plan-Do-Study-Act (PDSA) cycle as the foundational framework for our quality improvement initiative. This iterative model allowed us to systematically test changes in our healthcare delivery process, assess outcomes, and refine our approach based on real-time feedback.
To assess the impact of the implemented interventions, a mixed-methods approach was utilized. This included both quantitative and qualitative data collection methods. Quantitative Data included Appointment wait times, patient throughput, no-show rates, and patient satisfaction scores.
Measures
To evaluate the effectiveness of the quality improvement project at the Women’s Health Clinic, we focused on the following measures:
Outcome measure: Days to the next available appointment with a target of 14 days.
Process measures: Percentage of patients utilizing telehealth follow-ups (target > 20% National benchmark), number of patients seen per clinic session.
Balancing measure: Patient Satisfaction, which was measured through post-visit surveys assessing overall experience, including waiting times and quality of care.
Analysis
To evaluate the effectiveness of the interventions at the Women’s Health Clinic, we employed both qualitative and quantitative methods. For quantitative analysis, we collected numerical data on key metrics by using excel spread sheet, including appointment wait times, patient throughput, telehealth utilization rates, and no-show rates. Statistical analysis, such as descriptive statistics and trend analysis, was conducted to identify significant changes
In addition to quantitative methods, we implemented a qualitative approach through surveys to gain deeper insights into patient and staff experiences. Time-series analysis was used to track key metrics over time, enabling us to observe trends and fluctuations in response to the interventions. We also conducted segmentation analysis, breaking down the data weekly to assess the impact of the interventions at various stages. This approach helped distinguish immediate effects from long-term trends.
Ethical Considerations
An IRB approval was obtained on 23/07/2025 from the IRB committee at PSMMC with the number HP-01-R079.
Results
The project was scheduled to take place from mid-August to mid-September and successfully scheduled 900 virtual consultations within the one-month duration. Over this time, learning from each week, we continually improved on the service. The initial week revealed that physicians reported needing more training regarding the referral system, so another team meeting was conducted to provide more training and answering their questions. Patient feedback revealed some concerns regarding the possibility of missed diagnosis due to lack of physical exam; these concerns were addressed by explaining to each patient that a follow-up appointment and referral system are in place to ensure full clinical assessment and safety. Throughout the project, ongoing monitoring allowed timely adjustments. Weekly time TNAA, no-show rates, and patient feedback informed these adjustments. The project leader gradually increased the clinic capacity to meet the high demands at the Al-Wazarat centre (Table 1).
|
Table 1 Weekly Progression of Virtual Clinic Intervention and Key Performance Indicators |
||||
|
Week |
TNAA (days) |
No-Show Rate (%) |
Virtual Consultations (%) |
Key Interventions/Modifications Implemented |
|
Baseline (pre-project) |
75 |
30 |
0 |
N/A |
|
Week 1 |
60 |
25 |
40 |
Initial rollout of virtual assessments, physician re-training for referrals |
|
Week 2 |
40 |
20 |
55 |
Refinement of patient recall scripts |
|
Week 3 |
25 |
15 |
60 |
Communication protocol refined, tiered appointment system introduced |
|
Week 4 |
15 |
10 |
60 |
N/A |
TNAA: The time to the next available appointment; NA: Not Applicable
The intervention led to improvement in both process and outcome. Process improvement is represented in improved telehealth utilization, with 60% of patients receiving comprehensive assessment via the virtual consultation. This high rate of utilization was particularly useful to women who are in no need for a physical exam, like those who had a hysterectomy or have a medical history that exempts them from procedures like Pap smears (done within the last 3 years, or those aged above 65). By leveraging virtual services, we successfully addressed the specific needs of our patient population, allowing them to receive timely follow-up care without the necessity of in-person visits, as only 40% needed in-person visits (Figure 3). This not only streamlined the healthcare process for patients but also alleviated the burden on our clinic resources. Improved efficiency with average consultation time averaging 7-8 minutes, and optimization of scheduling helped to increase the number of patients seen from an average of 20 to 35-40 patients.
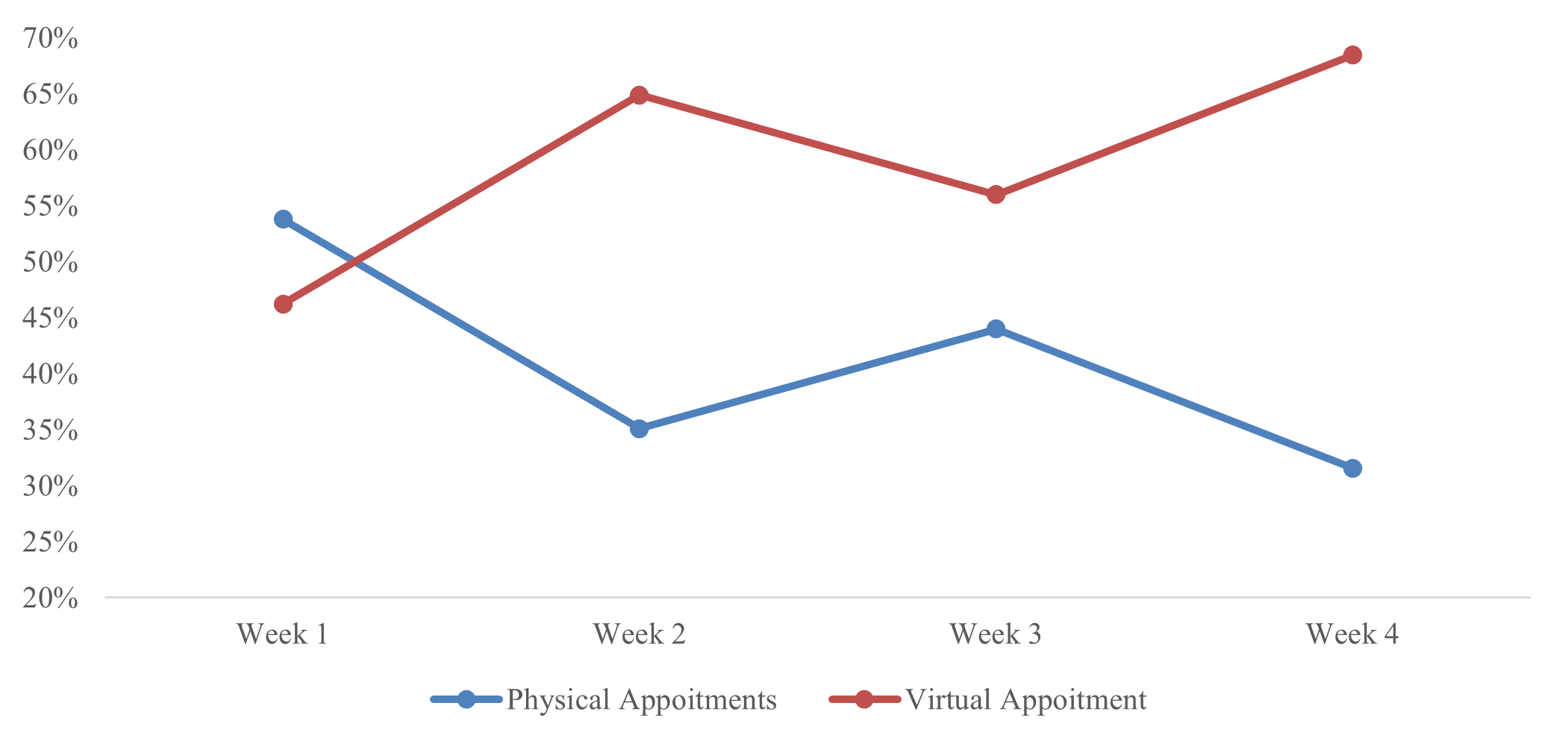
Figure 3: Percentage of virtual appointment vs physical visits.
Outcome measure improvement seen in reduced TNAA from 75 days to an average of 15 days (Figure 4), significantly improving appointment accessibility. Although the initial goal was to achieve a TNAA of 14 days, reaching 15 days still represents a substantial improvement in service delivery.
In addition, the no-show rate decreased compared to traditional face-to-face appointments from 30% before the implementation of the project to 10% at 4 weeks, indicating that telemedicine features enhanced patient compliance with scheduled sessions.
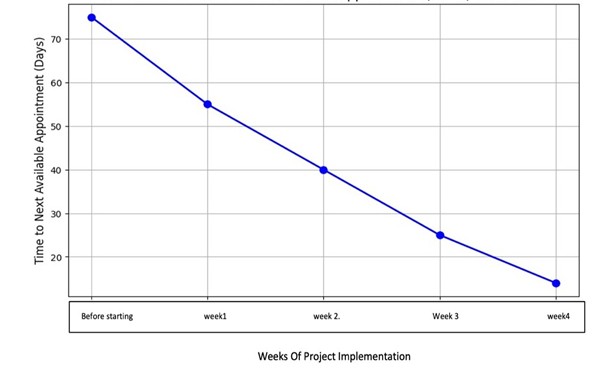
Figure 4: Next available appointment.
The graph in (Figure 5), illustrates patient satisfaction based on feedback collected at the end of each call, showing that the majority were satisfied. Over time, we have learned from each week and continuously improved the service.
Additionally, 85% of the feedback was positive, while only 15% was negative. We have taken these comments into account and worked on addressing them. Furthermore, all participating doctors expressed satisfaction with the virtual visits.
Figure 5: Patient satisfaction.
Despite the overall success, some unexpected outcomes and challenges were faced. Technical difficulties and inaccurate contact information on the system affected the service delivery and recall efforts. This is more pronounced with patients whose primary contacts are their fathers or husbands and those whose circumstances changed, like relocation or marriage. In contrast, an unexpected benefit observed was the satisfaction of participating physicians. The cost effectiveness highlighted by the reliance on existing resources and no external fundings were needed.
Efforts were made to ensure accurate and complete data. However, due to outdated contact information and the short duration of the project, this led to limitations in post-appointment surveys for some patients. We estimate the percentage to be 5% or less, and no imputation methods were undertaken due to the short duration of the project, and we focused on verified contacts to ensure strong, verifiable data.
Discussion
Results Summary
The quality improvement project at the Women’s Health Clinic successfully enhanced service delivery in women’s health through a virtual assessment model focused on preventive care. The intervention reduced the TNAA from 75 days to 15 days while improving patient experiences.
Key outcomes included a significant reduction in TNAA to 15 days, thereby improving access to healthcare. We achieved an 85% decrease in no-show rates and an 85% positive patient satisfaction rate. These results highlight the positive perceptions of virtual care and the effectiveness of our strategic interventions in appointment scheduling and telehealth.
Patient engagement also improved, with appointment confirmations rising to 85%. Notably, 60% of patients received comprehensive care through virtual appointments, with only 40% needing to reschedule for in-person visits.
A strength of the project was its mixed-methods approach, combining quantitative data analysis with qualitative feedback from patients and staff. This comprehensive assessment provided insights into the interventions’ effectiveness and identified areas for ongoing improvement. Despite some technical challenges, such as network connectivity issues, the project fostered a culture of continuous monitoring and adaptation, ensuring that changes remain relevant and effective over time.
In summary, the existing literature strongly supports the findings of our project. The reduction in TNAA and the increase in patient satisfaction observed in our study align with the documented benefits of telemedicine in both international and local contexts. This body of research highlights the importance of telehealth in addressing systemic challenges within women’s health services, ultimately promoting better health outcomes and improved patient experiences.
Results Interpretation
The quality improvement project at the Women’s Health Clinic demonstrated a strong positive correlation between the implemented interventions and the outcomes achieved. Notably, we observed an 85% decrease in no-show rates, an 85% positive patient satisfaction rate, and a 75% reduction in waiting times. These results indicate that the strategic changes, particularly in scheduling and telehealth implementation, directly enhanced patient access and overall experience.
Additionally, the integration of telemedicine into our healthcare delivery model has markedly expanded our operational capacity. Before the adoption of telehealth services, our facility managed an average of 320 patient encounters per month. With the implementation of telemedicine, this capacity has surged to 900 patient encounters per month, revealing a remarkable capacity increase of approximately 134% when excluding no-show patients. Importantly, a substantial proportion of these patient interactions were conducted remotely, allowing many patients to receive appropriate care without the necessity for in-person consultations. This shift not only enhances patient access to healthcare services but also optimizes resource allocation and reduces the burden on physical facilities, ultimately contributing to improved healthcare quality and patient satisfaction.
Our findings align well with existing literature. For instance, the importance of measuring appointment availability is highlighted as crucial for enhancing patient access. Our project succeeded in reducing the TNAA from 75 days to 15 day which corroborates findings from the study done by Pullyblank et.al., where the time for an in-person visit was 37 days and for video consultation was 19 days. (8) Additionally, Buchalter et al. and Donelan et al. both were able to demonstrate a high satisfaction rate with telehealth services. (4,5) The positive effects of telehealth on patient satisfaction are noted in our project, which is reflected in our high satisfaction scores. A systematic review confirms that telehealth interventions effectively reduce barriers to care and improve follow-up attendance. (6) This was also reported by Parajuli J. et al. (7). Both these findings mirror our project’s outcomes. There was a marked decrease in the no-show rate from 30% to 10% in our project supporting improved compliance with telehealth utilization. Pullyblank et al. have also reported similar findings, where in-person visits had 11.1% no-show rates compared to only 3.3% for remote follow-up visits. Furthermore, research supports the notion that streamlined processes can enhance clinic efficiency, while local healthcare dynamics are recognized as significant factors influencing patient engagement and outcomes. (5) In our project, this efficiency improvement can be seen in an increase in the number of patients per clinic from 20 to 35-40 per day. Our project is anchored in established frameworks that highlight the importance of accessibility and patient-centered care. While the project yielded largely favourable results, positively impacting patient outcomes and clinic workflows, some anticipated outcomes were not fully realized. By optimizing appointment scheduling and enhancing telehealth services, we improved operational efficiency within the clinic, benefiting the overall healthcare delivery system.
Limitations
While the project demonstrated significant improvements in patient access and engagement through the virtual care model, several limitations must be acknowledged. One major limitation was the reliance on contact information stored in the system, which was often inaccurate. Changes in patients’ circumstances, such as marriage or relocation, led to outdated or incorrect phone numbers, making it difficult to reach patients. This issue was particularly pronounced for patients whose primary contact numbers were those of a husband or father, which may not be consistently updated in the system.
Additionally, the project’s short duration of just one month offered limited insight into the long-term effects of the virtual clinic model. Future research should explore the durability of this intervention over time to better understand its sustainability and effectiveness. Variability in patient engagement may also be influenced by external factors, such as shifts in healthcare policies or seasonal changes.
Despite these mitigation efforts, the identified limitations highlight areas for further investigation to enhance the effectiveness and reliability of the virtual assessment care model.
Conclusions
The virtual clinic project clearly demonstrated the value of telehealth in enhancing access, patient satisfaction, and clinical outcomes. It successfully reduced waiting times from 75 to 15 days, decreased the percentage of no-show and achieved high patient satisfaction rates. Telehealth interventions also improved clinic efficiency and the management of chronic illnesses. Given these positive outcomes, further research should focus on provider training, technical assistance, and long-term evaluation of the program. This should include exploring the use of more advanced telehealth technologies. The virtual clinic model shows great promise and could be expanded to different healthcare contexts.
Acknowledgements
We are grateful for the assistance of the Quality Assurance Division at Prince Sultan Military Medical City, as their support has facilitated the completion of this project. We would also like to extend our thanks to the administrative assistants at the Al-Wazarat Centre.
Disclosure
Statement
The QI project was a local initiative developed by a multidisciplinary team of clinicians and administrators at Al-Wazarat Health Centre, Prince Sultan Military Medical City. Patient and public representatives were not involved in the design or execution of this specific initiative.
Funding
No funding.
Conflict of interest
There is no conflict of interest.
Ethical consideration
An Institutional Review Board approval was obtained on 23/07/2025 from the IRB committee at Prince Sultan Military Medical City with the number HP-01-R079.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.
Data availability
All data is available within the manuscript.