Volume 5, Issue 1
January 2025
The Subvastus Approach for Total Knee Arthroplasty in Obese Patients: A Systematic Review
Mohammed Daghistani, Samirah Alharbi, Taghreed Almohammadi, Anwar Sayed
DOI: http://dx.doi.org/10.52533/JOHS.2025.50102
Keywords: Arthroplasty, Obese patients, Replacement, Subvastus approach, Total knee
Total Knee Arthroplasty (TKA) represents a pivotal intervention in the management of advanced knee pathologies such as osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis. Various surgical approaches, including the subvastus, medial parapatellar, and midvastus techniques have evolved to optimize outcomes. While the subvastus approach offers potential advantages such as preserving the extensor mechanism and promoting early recovery, its applicability in obese patients remains a subject of debate due to challenges in exposure and patellar eversion. This systematic review explores the efficacy of the subvastus approach in obese patients, addressing both early and late outcomes, and discusses strategies to overcome exposure difficulties. A PRISMA systematic search appraisal was conducted. A systematic literature search of six scientific databases, including PubMed, Web of Science, SCOPUS, EMBASE, MEDLINE and Google Scholar, was conducted until April 20, 2024, to identify all relevant English-articles. Data was extracted from eligible studies. The literature search yielded a total of 983 studies. Eleven papers published from 2000 until 2021 met the inclusion criteria were included in the final analysis. The total number of patients throughout all the included studies was 1147. The main results showed that the subvastus approach for TKA is applicable in obese patients. To overcome its exposure difficulties, a multifaceted approach including preoperative weight management and advanced imaging could aid in optimizing patient selection and planning; furthermore, intraoperatively meticulous soft tissue handling, pneumatic tourniquets, and advancements like navigation systems could enhance exposure and precision; finally, specialized instruments and implants designed for minimally invasive techniques could improve outcomes. Overcoming exposure difficulties in the subvastus approach for TKA in obese patients demands a multifaceted approach blending preoperative planning, intraoperative techniques, and technological innovations. While challenges such as patellar eversion persist, innovative strategies like the mini-subvastus approach demonstrate efficacy in tackling these issues and ensuring successful outcomes in obese patients undergoing TKA.
Introduction
Total knee replacement (TKR), or Total Knee Arthroplasty (TKA) stands as a cornerstone in the surgical management of advanced knee diseases like osteoarthritis, rheumatoid arthritis, and posttraumatic arthritis. TKA is a common orthopaedic surgery that involves replacing the articular surfaces (femoral condyles and tibial plateau) of the knee joint with smooth metal and highly cross-linked polyethylene plastic (1). TKA aims to improve the quality of life of individuals by reducing pain and increasing function, plus it was found to improve patients' sports, physical activity and enhance patient outcomes (2). The most common indication for TKA is osteoarthritis (1). Osteoarthritis causes the cartilage of the joint to become damaged and no longer able to absorb shock. Risk factors for knee osteoarthritis include gender, increased body mass index, history of knee injury and comorbidities (1, 2).
During the surgery: 1) there is at least one polyethylene piece, placed between the tibia and the femur as a shock absorber; 2) the prostheses are usually reinforced with cement, but may be left uncemented where bone growth is relied upon to reinforce the components; 3) the patella may be replaced or resurfaced (patella reconstruction aims to restore the extensor mechanism); 4) a quadriceps-splitting or quadriceps-sparing approach may be used; and 5) the cruciate ligaments may be excised or preserved (3). TKA is a reliable surgical procedure with a predictable outcome in the appropriate patient. In addition, the reported survival rates are upward of 85% with 10 to 25 years of follow-up (4). Damaged bone, cartilage, and ligaments cannot heal on their own; in some cases, knee joints may begin to deteriorate and eventually lose function altogether if left untreated, creating even more pain (5).
Various surgical approaches, including the subvastus, medial parapatellar, and midvastus, have evolved to access and implant prosthetic components within the knee joint (3). The classic medial parapatellar approach involves a medial incision through the quadriceps muscles, providing excellent exposure but potentially compromising patellar vascularity and function (2). Alternatively, the midvastus approach offers improved early range of motion but at the expense of longer operative times (3,4). Furthermore, the subvastus approach has gained traction due to its potential benefits, including maintaining the extensor mechanism, enhancing patellar tracking, and promoting earlier quadriceps recovery. The subvastus surgical technique to the knee joint includes removing the vastus medialis muscle from its femur origin before dislocating the patella laterally, leaving the quadriceps mechanism intact (5). Despite its advantages, concerns persist regarding its application in obese patients, who often pose surgical challenges such as inadequate visualization and patellar eversion difficulties (6).
Obesity has become a pressing global health concern, with its prevalence steadily rising over the years. In 2022, 2.5 billion adults (18 years and older) were overweight. Of these, 890 million were living with obesity (7). In fact, the more weight obese patients carry around, whether it is muscle or fat, the greater the load on their hips and knees. This is one reason why heavier people are more likely to require total hip and knee replacements than patients with normal body mass index (BMI), and why the risk increases as the BMI increases (8). Additionally, the surge in obesity presents various challenges, particularly in healthcare, such as performing TKA procedures (9). Obese individuals undergoing TKA face heightened risks of complications including infection, delayed wound healing, and prosthetic failure (9, 10). Additionally, excessive body weight places greater stress on the replaced joint, potentially leading to early implant loosening and reduced longevity of the prosthetic joint (9, 10).
In this systematic review, we explore the efficacy of the subvastus approach in obese patients, examining both early and late outcomes. We also review the impact of factors such as surgeon experience, patellar tracking, and modified techniques tailored to address challenges encountered in obese populations. Through this review, we aim to provide insights into optimizing surgical strategies and improving outcomes in obese patients undergoing TKA with the subvastus approach.
Methodology
Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) systematic search appraisal was conducted using a combination of keywords including "knee replacement," OR "knee arthroplasty," AND "obese patients,” OR "high BMI," OR "large thigh girth," AND "subvastus approach," OR "southern approach." A systematic literature search of six scientific databases, including PubMed, Web of Science, SCOPUS, EMBASE, MEDLINE and Google Scholar were conducted until April 20, 2024, to identify all relevant articles. Eleven articles published from 2000 until 2021 met the inclusion criteria of the current systematic review.
Eligibility Criteria
This analysis collected all original English-language articles with various study designs (Randomized controlled study, case control study, retrospective cohort study, and cross-sectional study) on the efficacy of the subvastus approach for TKA in obese patients. Titles and abstracts of retrieved articles were screened for relevance, excluding studies unrelated to the subvastus approach in TKA, articles not written in English, and reviews or editorials. The remaining articles underwent full-text review, and data pertaining to the applicability of the subvastus approach in obese patients were extracted for analysis.
Data Extraction
The study authors separately evaluated the titles and abstracts of the articles for relevance in accordance with the inclusion criteria listed above after eliminating duplicates. The study authors individually evaluated the full texts of the chosen papers to determine if they were appropriate for the current review. The discussion was carried out to settle any disputes. Data from the included articles were extracted for evidence synthesis using a standardized Excel sheet. The first author, publication year, study design, and outcomes were all extracted.
Assessment of Quality
A modified version of the National Institutes of Health Quality Assessment tool, which addresses the design, selection bias, data collection, confounders, blinding, and attrition was used to evaluate the quality of the qualifying papers. An overall grade of 'good', 'fair', or 'poor' was provided for each article (11).
Results
Databases Searching and Articles Inclusion Process
A total of 983 articles were identified in the database search process. After the removal of duplicates, 312 articles remained. 116 articles were excluded by title screening, 140 articles were excluded by abstract screening, the full text of the remaining 56 articles was assessed for eligibility, and 45 articles were removed for reasons mentioned in (Figure 1). Eventually, 11 articles published from 2000 until 2021 met the inclusion criteria of the current systematic review.
Characteristics of the Eligible Articles
In the current systematic review, only papers with good methodological quality were included. Out of the 11 included articles (12-22), two articles were published in 2013 (13,15), 4 were published in 2010 (12, 16, 18, 22), and 1 was published in each year; 2021, 2017, 2016, 2005, and 2000 (14, 17, 19, 20, 21). In addition, 4 articles were randomized controlled trials (12, 15, 18, 22), 2 articles were retrospective cohort (14, 21), 3 articles were case control (13, 19, 20), and the remaining 2 articles where cross-sectional (16, 17). The total number of patients throughout all the included studies was 1147 (Table 1). Moreover, Table 2 shows the main outcomes of the included articles.
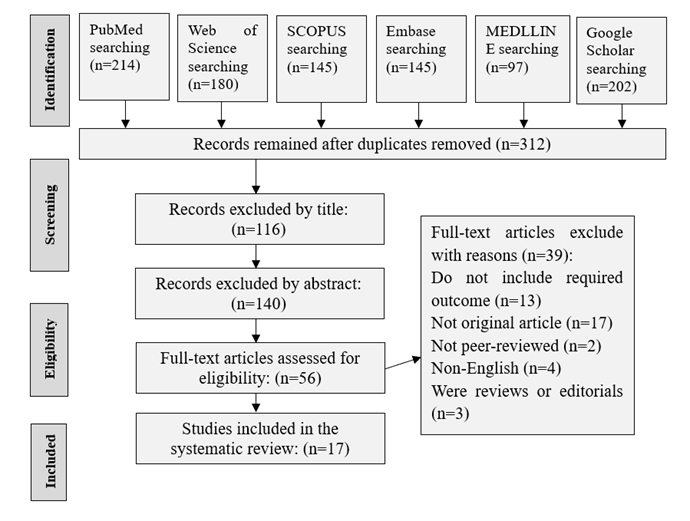
Figure 1: PRISMA chart of the databases searching and articles inclusion process.
|
Table 1: Characteristics of eligible articles |
||||
|
First author |
Journal |
Publication year |
Study design |
Number of patients in the studies |
|
Van Hemert et al. (12) |
Knee Surg Sports Traumatol Arthrosc |
2010 |
Randomized controlled study |
40 patients |
|
Pongcharoen et al. (13) |
Clin Orthop Relat Res. |
2013 |
Case control study |
59 patients (60 knees; with 30 cases and 30 control group) |
|
Shah et al. (14) |
Indian J Orthop. |
2016 |
Retrospective cohort study |
84 patients |
|
Jain et al. (15) |
Indian J Orthop. |
2013 |
Randomized controlled study |
100 patients |
|
Shah et al. (16) |
Indian J Orthop. |
2010 |
Cross-sectional study |
97 patients |
|
Kekatpure et al. (17) |
Reconstructive Review |
2017 |
Cross-sectional study |
88 patients |
|
Varela-Egocheaga et al. (18) |
Clin Orthop Relat Res. |
2010 |
Randomized controlled study |
100 patients |
|
Sood et al. (19) |
Journal of Research and Practice |
2021 |
Case control study |
100 patients (50 cases and 50 control group) |
|
Boerger et al. (20) |
Clin Orthop Relat Res. |
2005 |
Case control study |
120 patients (60 cases and 60 control group) |
|
Matsueda and Gustilo (21) |
Clin Orthop Relat Res. |
2000 |
Retrospective cohort study |
291 patients |
|
Pan et al. (22) |
J Int Med Res. |
2010 |
Randomized controlled study |
68 patients |
|
Table 2: Outcomes of the eligible articles |
|
|
First author |
Study outcomes |
|
Van Hemert et al. (12) |
Only mild advantage (an early extension lag functioning was in favor of the subvastus approach) employing the subvastus approach was found, but only early postoperative and not objectively, and this approach is not suitable in every case. No difference was found between the parapatellar approach and subvastus approach in terms of pain reduction and restoration of function, and both have anatomical disadvantages. |
|
Pongcharoen et al. (13) |
Minimally invasive surgical TKA using either the medial parapatellar or midvastus approach has a low incidence of patellar maltracking and anterior knee pain. |
|
Shah et al. (14) |
Satisfactory results of TKA can be obtained in knees with limited preoperative range of motion using subvastus approach maintaining the advantages of early mobilization. |
|
Jain et al. (15) |
Subvastus approach produces appreciably less pain and faster mobilization due to lesser insult to quadriceps, thus assisting in early rehabilitation, shorter hospital stay, less expenditure, and more patient satisfaction. |
|
Shah et al. (16) |
The authors concluded that the mini-subvastus approach can be considered in obese patients. |
|
Kekatpure et al. (17) |
The mini-subvastus approach can be considered for TKA in obese and morbidly obese patient population with outcomes comparable to standard surgical approach. |
|
Varela-Egocheaga et al. (18) |
The minimally invasive subvastus approach can result in improved long-term Knee Society scores and range of motion of total knee arthroplasty without increased risk of component malalignment, surgical time, or complication rate. |
|
Sood et al. (19) |
Subvastus approach had less post-operative pain, faster recovery and better functional outcomes after surgery as compared to medial para-patellar approach in early post-operative period. In addition, the subvastus approach significantly improves early outcomes in simultaneous bilateral total knee arthroplasty cases. |
|
Boerger et al. (20) |
The mini-subvastus approach offers early but short-lived benefits for patients at the expense of a longer operation and a higher risk of complications. |
|
Matsueda and Gustilo (21) |
The authors concluded that the subvastus approach led to improved patellar tracking and stability. |
|
Pan et al. (22) |
The authors showed that patients who use the mini-subvastus approach for minimally invasive TKA lost less blood and experienced less pain post-operatively. They achieved an active straight leg raise earlier, underwent less lateral retinacular releases, and the range of knee movements were better post-operatively. In contrast, reduced access and visibility in patients who use the mini-subvastus approach prolonged the operation time and resulted in five technical errors on radiographic evaluation. Based on these results, the authors currently only use the mini-subvastus approach for minimally invasive TKA. |
TKA: Total Knee Arthroplasty; BMI: Body Mass Index
Discussion
This systematic review explores the efficacy of the subvastus approach in obese patients, addressing both early and late outcomes, and discusses strategies to overcome exposure difficulties. The main findings of this systematic review showed that in recent years, technological advancements have played a significant role in overcoming exposure difficulties in obese patients undergoing TKA via the subvastus approach. Navigation systems and robotic-assisted surgery offer enhanced precision and accuracy, allowing surgeons to navigate through complex anatomical structures with greater ease, even in cases of limited exposure due to obesity. These technologies provide real-time feedback and guidance, enabling surgeons to make informed decisions and optimize implant placement while mitigating the challenges associated with poor visualization. Furthermore, the development of specialized instruments and implants designed specifically for minimally invasive techniques has improved the feasibility and outcomes of TKA in obese patients. For instance, angled retractors and custom-made instruments enable surgeons to work within confined spaces and achieve adequate exposure while minimizing soft tissue trauma. Additionally, the use of smaller incisions and tissue-sparing approaches reduces the extent of surgical trauma and accelerates postoperative recovery, particularly in obese patients who may be at higher risk of wound complications and delayed healing.
Preoperative Measures
Preoperative weight loss programs, when feasible, can help reduce adipose tissue around the knee joint, improving exposure and facilitating the surgical procedure (23, 24). Additionally, advanced imaging techniques such as magnetic resonance imaging or computed tomography scans can provide valuable information about the distribution of adipose tissue and aid in surgical planning (25).
Intraoperative Exposure
Obesity presents unique challenges in TKA, including limited exposure of the surgical site, difficulty in achieving adequate soft tissue balance, increased risk of wound complications, and potential for suboptimal outcomes. Intraoperative exposure in TKA for obese patients is a critical consideration due to the challenges posed by increased adipose tissue and altered anatomy. Among the various surgical approaches, the subvastus approach has gained attention for its potential to provide improved exposure while minimizing muscle damage and postoperative pain (16). The subvastus approach is considered an anatomic technique because it avoids disruption of the quadriceps tendon and the insertion of the vastus medialis (26). However, there are some considerations when using the subvastus approach in obese patients.
Obesity can pose challenges in terms of exposure during the subvastus approach. The difficulty in exposure and eversion of the patella can make the subvastus approach a contraindication in obese patients (16). Additionally, increasing obesity, as indicated by higher thigh girth measurements, can lead to more significant difficulties in exposure and a higher incidence of peri-operative complications with the subvastus approach (17). In some cases, knee exposure may be inadequate, especially in obese patients with excessive thigh girth and stiff knees (18). However, it is essential to note that the subvastus approach has been used successfully in obese patients. A study comparing outcomes in elderly obese patients undergoing simultaneous bilateral TKA using the subvastus approach found no significant differences in body mass index and gender compared to the medial para-patellar approach (19). Another study focused on elderly non-obese patients undergoing bilateral simultaneous TKA and found positive outcomes with the subvastus approach (27).
A previous study evaluated various surgical approaches in TKA for obese patients and found that the subvastus approach was associated with reduced postoperative pain and improved early functional outcomes compared to other techniques. The authors highlighted the importance of minimizing soft tissue trauma in this patient population to facilitate rehabilitation and optimize long-term results. In terms of clinical outcomes, the subvastus approach has shown promising results (12). A meta-analysis comparing the subvastus and medial parapatellar approaches found no significant differences in blood loss, surgical time, or postoperative range of motion (28).
In addition to preserving muscle function, the subvastus approach offers potential advantages in wound healing and infection risk reduction. By avoiding a midline incision and minimizing soft tissue dissection, this approach may reduce the risk of wound complications in obese patients, who are already predisposed to such issues due to impaired vascularity and increased microbial load in adipose tissue (16, 29). Despite these potential benefits, challenges still exist in achieving optimal intraoperative exposure in obese patients undergoing TKA via the subvastus approach. The thickness of adipose tissue and altered anatomy can make identification and dissection of anatomical landmarks more challenging, requiring careful surgical technique and possibly specialized instrumentation (16).
Postoperative Outcomes of the Subvastus Approach for TKA
The subvastus approach for TKA has garnered significant interest in recent years due to its potential benefits in postoperative outcomes compared to traditional approaches, such as the medial parapatellar approach. This surgical technique involves a smaller incision and preserves the quadriceps mechanism, specifically the vastus medialis obliquus (VMO), which is hypothesized to lead to faster recovery, improved range of motion, and reduced postoperative pain (30). While its adoption has increased, the evidence regarding its superiority over traditional approaches remains a topic of debate within the orthopaedic community. Numerous studies have investigated the postoperative outcomes of the subvastus approach, with varying conclusions. One of the main advantages reported is a reduced incidence of postoperative quadriceps weakness, leading to faster recovery of quadriceps strength and function (30-32). This is attributed to the preservation of the VMO attachment, which helps maintain the integrity of the extensor mechanism of the knee. Additionally, proponents of the subvastus approach suggest that it may result in less postoperative pain and reduced need for analgesics, contributing to improved patient satisfaction and earlier mobilization (31, 32).
A systematic review by Hofmann et al. (5) compared the subvastus approach to the medial parapatellar approach and found that patients undergoing TKA with the subvastus approach had significantly better outcomes in terms of quadriceps strength, range of motion, and functional scores in the early postoperative period. However, the difference in outcomes diminished over time, suggesting that any initial advantages may not be sustained in the long term. A meta-analysis also showed that the subvastus approach had significant advantages over the standard approach in visual analog score, range of motion, straight leg raises and lateral retinacular release, and no disadvantages were found associated with the subvastus approach (26).
In terms of postoperative complications, a previous study reported lower rates of anterior knee pain and decreased risk of patellar mal-tracking with the subvastus approach (13). However, other complications such as wound complications, intraoperative fractures, and prolonged operative times have also been associated with this technique, albeit at varying rates across studies (14, 15). While the subvastus approach offers potential benefits, it is important to consider its limitations. Surgeon experience and patient selection play crucial roles in achieving favourable outcomes with this technique. Moreover, the subvastus approach may not be suitable for all patients, particularly those with severe deformities or extensive soft tissue contractures.
Patella Tracking
Patellar tracking is defined as the motion of the patella relative to the femur or femoral groove on knee flexion and extension. In addition, patella tracking in TKA is a critical aspect of ensuring optimal function and longevity of the implant (33). Obesity is a well-established risk factor for complications in TKA, including poor patellar tracking, increased rates of postoperative infection, and decreased functional outcomes (34). In obese patients, achieving proper patellar tracking becomes even more crucial. The excessive soft tissue and adipose tissue can hinder surgical exposure and lead to difficulties in achieving optimal patellar tracking. Traditional approaches to TKA may exacerbate these issues by disrupting the extensor mechanism and compromising patellar stability (35). The subvastus approach in TKA offers potential advantages in addressing these challenges in obese patients (12).
By avoiding disruption of the quadriceps tendon and patella, the subvastus approach minimizes the risk of patellar mal-tracking and subsequent complications (20). In obese patients, this approach firstly reduces the disruption of soft tissue as it involves a smaller incision and less dissection of soft tissue compared to traditional approaches (16, 21). This preservation of soft tissue integrity can help maintain the structural support around the patella, reducing the risk of lateral displacement or tilt. Secondly, it improves patellar tracking by sparing the quadriceps tendon and avoiding excessive manipulation of the patella and promoting more physiological patellar tracking (12, 22). This may lead to better functional outcomes and decreased rates of complications such as anterior knee pain and instability. Lastly, it enhances postoperative rehabilitation. Obese patients often face challenges in postoperative rehabilitation due to limited mobility and increased risk of wound complications. The minimally invasive nature of the subvastus approach may facilitate earlier mobilization and rehabilitation, promoting faster recovery and improved outcomes (18).
Several studies have investigated the impact of the subvastus approach on patellar tracking and clinical outcomes in obese patients undergoing TKA. A recent meta-analysis by Migliorini et al. (35) analysed data from multiple studies and found that the subvastus approach was associated with lower rates of patellar mal-tracking and improved functional outcomes compared to traditional approaches in obese patients. Similarly, the subvastus approach in total knee arthroplasty has been associated with improved patellar tracking and stability compared to the standard medial parapatellar approach (36). By preserving the VMO insertion on the patella, the subvastus approach helps maintain the integrity of the medial supporters of the patella, leading to better patellar tracking (16, 36). This preservation of the VMO insertion allows for better postoperative quadriceps control and strength, further contributing to improved patellar tracking (1). In contrast, the medial parapatellar approach involves dividing the medial supporters of the patella, making it more challenging to assess patella-femoral tracking (16). The subvastus approach, on the other hand, allows for a more straightforward evaluation of the tracking of the patella-femoral joint due to the intact medial supporters of the patella (16).
Overcoming Exposure Difficulties in Subvastus Approach in Obese Patients
Overcoming exposure difficulties in the subvastus approach for TKA in obese patients presents a significant challenge for orthopaedic surgeons. One of the primary challenges in obese patients undergoing TKA via the subvastus approach is limited visualization of the surgical field due to excess soft tissue (16, 37). Several studies have highlighted the importance of preoperative planning and patient optimization in addressing this issue (29). Preoperative weight loss programs, when feasible, can help reduce adipose tissue around the knee joint, improving exposure and facilitating the surgical procedure (23, 24). Additionally, advanced imaging techniques such as magnetic resonance imaging or computed tomography scans can provide valuable information about the distribution of adipose tissue and aid in surgical planning (25).
During the surgical procedure, specific techniques can be employed to enhance exposure and improve visualization in obese patients. Utilizing pneumatic tourniquets can help reduce blood loss and improve visualization by minimizing intraoperative bleeding, particularly in obese patients who are at increased risk of intraoperative haemorrhage (38). Moreover, careful soft tissue dissection and meticulous haemostasis are crucial to optimize exposure while minimizing damage to surrounding structures. One study suggested that the patella could only be everted after the femoral and tibial cuts had been made. Subsequently, hypertrophic suprapatellar synovium and overhanging osteophytes from the patella can be easily removed after everting the patella (17). The mini-subvastus approach provided satisfactory exposure in all knees that were operated. The approach proved equally effective in the knees that were expected to be difficult, i.e., morbidly obese patients with large thigh girth (above 55 cm) irrespective of any degree of varus or valgus deformity. Patellar eversion and tibiofemoral dislocation prior to bony cuts are also avoided (16).
Strengths and Limitations
The strength of this systematic review is that, to our knowledge, it is one of the few studies, which shows the efficacy of the subvastus approach in obese patients undergoing TKA and examining both early and late outcomes. The present systematic review may provide baseline data on the efficacy of the subvastus approach in obese patients undergoing TKA and can guide other researchers to design new studies. On contrary, the current systematic review is prone to some limitation including the articles published in languages other than English were excluded.
Conclusion
The subvastus approach for TKA is applicable in obese patients and is linked to a faster recovery. Overcoming exposure difficulties in the subvastus approach for TKA in obese patients demands a multifaceted approach blending preoperative planning, intraoperative techniques, and technological innovations. While challenges such as patellar eversion persist, innovative strategies like the mini-subvastus approach demonstrate efficacy in tackling these issues, ensuring successful outcomes in obese patients undergoing TKA.
Disclosure
Statement
The authors declare no conflict of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Consideration
Not applicable.
Data Availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contribution
MD and SA collected, analysed, extracted and interpreted the data and wrote the first draft of the manuscript. MD, SA, TA, and AS significantly contributed in the study design and the critical review of the manuscript. MD remarkably contributed to the analysis and interpretation of data and the critical review of the manuscript. All authors contributed to the article and approved the submitted version.
