Volume 4, Issue 12
December 2024
Prevalence and Predictors of Burnout Among Healthcare Workers of Palliative Care Department in King Fahad Medical City, Riyadh, Saudi Arabia
Ahmad Khalifah AlKhalifah, Reem Sulaiman Alsalman, Maied Zaher AlShehery
DOI: http://dx.doi.org/10.52533/JOHS.2024.41215
Keywords: Burnout, Healthcare workers, Palliative care, Saudi Arabia
Background: The need for providing palliative care is increasing worldwide because of the progression in life expectancy accompanied by advances in medical care and having many patients with incurable and advanced diseases. This is mostly accompanied by a stressful life for health workers, as they face daily tragedy and suffering; therefore, they are at higher risk for burnout. The current study was conducted to estimate the rate and associated factors of burnout and its dimensions among healthcare workers of the Palliative Care Department in King Fahad Medical City, Riyadh, Saudi Arabia.
Methodology: This observational cross-sectional study was performed at the palliative care department in King Fahad Medical City, Riyadh, Saudi Arabia, among all healthcare workers. Data was collected using a pre-designed, valid self-administrated questionnaire. It included two main sections: sociodemographic and work-related data and Maslach burnout inventory (MBI) to assess the overall burnout and its three subscales: emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA).
Results: The prevalence of high EE was 49.3%, whereas those of high DP and low PA were 62% and 63.4%, respectively. The overall prevalence of burnout among palliative care health workers was 23.9%. Multivariate logistic regression analysis revealed that divorced/widowed participants were at a significantly higher risk of burnout compared to singles, with adjusted odds ratio (AOR) =18.92; 95% confidence interval (CI) 2.63-136.14, p=0.004. Compared to participants with short annual vacations (★4 weeks), those with long annual vacations (>4 weeks) were at lower risk for burnout (AOR=0.27; 95% CI: 0.08-0.84), p=0.024.
Conclusion: Burnout is a prevalent problem among healthcare workers working in palliative care in Riyadh, with no difference between physicians, nurses, and other workers. Decision makers should take care of the working environment of this category of healthcare, particularly their annual vacation length, and specific attention should be given to divorced/widowed workers to reduce the burden of burnout among them.
Introduction
Burnout is a common problem affecting healthcare professionals, who often experience burnout at a higher rate compared to the general population, which is mostly attributed to work-related stress (1, 2). Burnout is a complex process that includes three dimensions; high emotional exhaustion (EE), high depersonalization (DP), and low personal accomplishment (PA), and its severity ranges from being absent to severe symptoms (3, 4).
The need for providing palliative care is increasing worldwide because of the progression in life expectancy accompanied by advances in medical care and having many patients with incurable and advanced diseases (5). This palliative care is characterized by a multidisciplinary need for psychological, spiritual, physical, as well as environmental holistic care for patients and their caregivers aimed at achieving “death with dignity” (1).
The increasing need for palliative care is mostly accompanied by stressful life for health workers as they daily face tragedy and suffering; therefore, they are at higher risk for burnout (6). Burnout symptoms among healthcare workers not only affect their well-being but are also associated with poor quality of care delivered to patients and an increase in the risk of making errors (7, 8). Furthermore, burnout has been associated with higher rates of job turnover, absenteeism, and decreased productivity as well as job dissatisfaction (9), which consequently leads to shortages of healthcare workers and increased demand for them (10). Therefore, preventing burnout among healthcare workers in general, and those working in palliative care in particular through training in communication skills, meditation, mindfulness, and self-care efforts is vital to maintaining adequate quality of care (11, 12).
Some studies have been carried out in the last decade to estimate the prevalence and define determinants of burnout among healthcare workers involved in palliative care; mainly in Western countries and Asia (2, 13-15), and only one recent study has been conducted in the Kingdom of Saudi Arabia (16).
Burnout is a serious worldwide problem impacting considerably healthcare staff working in palliative care, who often must deal with end-of-life complex situations. Despite that, the issue is not sufficiently investigated in the Kingdom of Saudi Arabia. Therefore, more studies are needed to identify the magnitude as well as associates of the problem among them and look for applicable solutions to overcome this problem that affects negatively the quality of life, work performance, as well as retention of affected individuals. The current study aims to explore the magnitude and associated factors of the problem of burnout among healthcare workers in palliative care and recommend possible solutions to manage the problem.
Methodology
Study design and settings
This was an observational cross-sectional design performed at the Palliative Care Department in King Fahad Medical City, Riyadh, Saudi Arabia.
Sample size calculation method
All healthcare workers of the Palliative Care Department in King Fahad Medical City (physicians, nurses, and others) were included in the study with no specific exclusion criteria. The estimated number was 166 (25 physicians, 129 nurses, and 12 others (social workers, nutritionists, and physiotherapists).
Data collection instrument and technique
Data was collected using a pre-designed, valid self-administrated questionnaire. It included two main sections: sociodemographic and work-related data: age, sex, nationality, job title, duration of work in the current healthcare facility, number of working days per week, duration of annual vacation in days and on call history, and Maslach burnout inventory (MBI). It includes 22 statements that assess the overall burnout and its three subscales: emotional exhaustion (EE) = 9 items, depolarization (DP) (cynicism) = 5 items, and personal achievement (PA) = 8 items. For the EE and DP subscales, higher mean scores correspond to a higher degree of burnout, while for the PA subscale, a lower mean score means a higher degree of burnout.
Respondents were asked to express their responses for each statement on a 7-point Likert scale (ranging from 0 ''never'' to 6 "every day"). The scores for each subscale were considered separately and were not combined into a single total score; thus, three scores were computed for each respondent. High EE was considered at a score of ≥27, high DP was considered at a score of >10, and low PA was considered at a score of <33. Burnout was defined as high scores in EE and DP and low scores in PA (17).
Ethical consideration
All the required official approvals, particularly the approval of the local Research and Ethics committee at King Fahad Medical City, Riyadh, were fulfilled. Permissions from the medical director and head of the Palliative Care Department of King Fahad Medical City were requested. A written consent was taken from all participants after explaining the objectives of the study to them in a short sentence before the questionnaire. Confidentiality and privacy were maintained throughout all steps of the research.
Statistical analysis
Data was collected and verified by hand and then coded before computerized data entry. The Statistical Package for Social Sciences (SPSS) software version 28.0 was used for data entry and analysis. Descriptive statistics (e.g. number, percentage, mean, range, standard deviation "SD") and analytic statistics using the chi-square test (χ2) and independent two-sample t-test were applied. Multivariate logistic regression analysis expressed as adjusted odds ratio (AOR) and 95% confidence interval (CI) was used to determine predictors of burnout after controlling for the confounding effect and p-values ≤0.05 were considered statistically significant throughout the study.
Results
Response rate
Out of 166 healthcare providers targeted to participate in the study, 142 responded by filling out the study questionnaire completely, giving a response rate of 85.5%.
Sociodemographic and work-related characteristics
A total of 142 palliative care health workers were included in the study. Their sociodemographic and work-related characteristics are summarized in Table 1. Males represented 54.9% of them. Their age ranged between 23 and 59 years with a mean of 36.2 ± 8.5 years. Regarding their marital status, 70.5% were married, whereas 23.9% were singles. More than half of them (56.3%) were Saudi nationals. Nurses represented most of them (76.8%). More than half of them (57%) worked for 5 years or less, whereas 16.2% worked for more than 10 years in the current healthcare facility. The majority of them (80.3%) work typically for 5 days per week. The duration of the annual vacation was 4 weeks or less among 69% of the respondents. On-call duties were reported by 74.6% of them.
Burnout
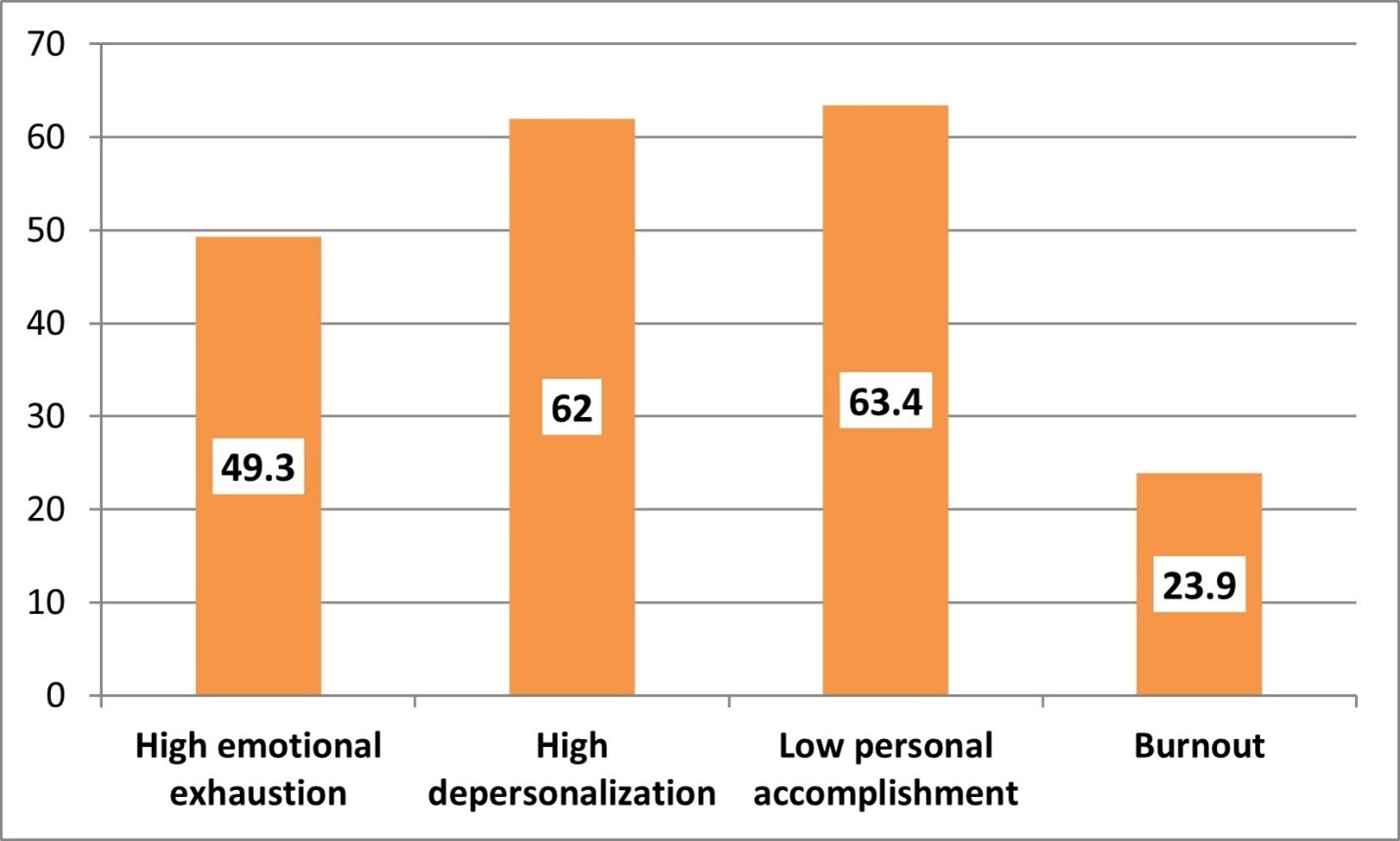
As demonstrated in Figure 1, the prevalence of high EE was 49.3%, whereas those of high DP and low PA were 62% and 63.4%, respectively. The overall prevalence of burnout among palliative care health workers was 23.9%.

Figure 1: Prevalence of high emotional exhaustion, high depolarization and low personal achievement among the study participants (n=142)
|
Table 1: Sociodemographic and work-related characteristics of the participants (n=142) |
||
|
Variables |
Frequency |
Percentage |
|
Gender Male Female |
78 64 |
54.9 45.1 |
|
Age (years) Range Mean ± SD |
23-59 36.2±8.5 |
|
|
Marital status Single Married Divorced/widowed |
34 100 8 |
23.9 70.5 5.6 |
|
Nationality Saudi Non-Saudi |
80 62 |
56.3 43.7 |
|
Job title Physician Nurse Others* |
25 109 8 |
17.6 76.8 5.6 |
|
Duration of work in the current healthcare facility (years) ≤5 6-10 >10 |
81 38 23 |
57.0 26.8 16.2 |
|
Typical number of working days/week ≤4 5 >5 |
10 114 18 |
7.0 80.3 12.7 |
|
Duration of annual vacation (weeks) ≤4 >4 |
98 44 |
69.0 31.0 |
|
On call duties No Yes |
36 106 |
25.4 74.6 |
SD: Standard deviation, *Social workers, nutritionists, and physiotherapists
Factors associated with burnout and its components
Emotional exhaustion
Among various studied sociodemographic and work-related factors, the only factors significantly associated with high EE were marital status and on-call duties. All divorced/widowed participants reported high EE compared to 48% and 41.2% of married and single participants, respectively; p=0.010. Participants without on-call duties were more likely than their peers to report high EE (72.2% versus 41.5%), p=0.001. Other studied sociodemographic and work-related factors were not significantly associated with high EE (Table 2).
|
Table 2: Factors associated with high emotional exhaustion among the study participants (n=142) |
|||
|
Emotional exhaustion |
p-value |
||
|
Low/medium (n=72) N (%) |
High (n=70) N (%) |
||
|
Gender Male (n=78) Female (n=64) |
38 (48.7) 34 (53.1) |
40 (51.3) 30 (46.9) |
0.601* |
|
Age (years) Mean ± SD |
35.4±8.1 |
37.0 ± 8.9 |
0.252° |
|
Marital status Single (n=34) Married (n=100) Divorced/widowed (n=8) |
20 (58.8) 52 (52.0) 0 (0.0) |
14 (41.2) 48 (48.0) 8 (100) |
0.010* |
|
Nationality Saudi (n=80) Non-Saudi (n=62) |
43 (53.8) 29 (46.8) |
37 (46.2) 33 (53.2) |
0.410* |
|
Job title Physician (n=25) Nurse (n=109) Others* (n=8) |
15 (60.0) 55 (50.5) 2 (25.0) |
10 (40.0) 54 (49.5) 6 (75.0) |
0.225* |
|
Duration of work in the current healthcare facility (years) ≤5 (n=81) 6-10 (n=38) >10 (n=23) |
45 (55.6) 18 (47.4) 9 (39.1) |
36 (44.4) 20 (52.6) 14 (60.9) |
0.143* |
|
Typical number of working days/week ≤4 (n=10) 5 (n=114) >5 (n=18) |
6 (60.0) 58 (50.9) 8 (44.4) |
4 (40.0) 56 (49.1) 10 (55.6) |
0.730* |
|
Duration of annual vacation (weeks) ≤4 (n=98) >4 (n=44) |
48 (49.0) 24 (54.5) |
50 (51.0) 20 (45.5) |
0.540* |
|
On call duties No (n=36) Yes (n=106) |
10 (27.8) 62 (58.5) |
26 (72.2) 44 (41.5) |
0.001* |
*Chi-square test, °Independent two samples t-test, SD: standard deviation
High depersonalization
All divorced/widowed participants reported high DP compared to 54% and 76.5% of married and single participants, respectively; p=0.005. The majority (87%) of participants who worked for more than 10 years in the current healthcare facility compared to 54.3% of those work for 5 years or less expressed high DP, p=0.017. Participants who had shorter annual vacations (≤4 weeks) were more likely than those with longer vacations (>4 weeks) to report high DP (71.4% versus 40.9%), p=0.001. Other studied sociodemographic and work-related factors were not significantly associated with high DP (Table 3).
|
Table 3: Factors associated with high depersonalization among the study participants (n=142) |
|||
|
Depersonalization |
p-value |
||
|
Low/medium (n=54) N (%) |
High (n=88) N (%) |
||
|
Gender Male (n=78) Female (n=64) |
26 (33.3) 28 (43.8) |
52 (66.7) 36 (56.2) |
0.203* |
|
Age in years Mean ± SD |
37.2±9.2 |
35.6±8.0 |
0.253° |
|
Marital status Single (n=34) Married (n=100) Divorced/widowed (n=8) |
8 (23.5) 46 (46.0) 0 (0.0) |
26 (76.5) 54 (54.0) 8 (100) |
0.005* |
|
Nationality Saudi (n=80) Non-Saudi (n=62) |
31 (38.8) 23 (37.1) |
49 (61.3) 39 (62.9) |
0.840* |
|
Job title Physician (n=25) Nurse (n=109) Others (n=8) |
13 (52.0) 37 (33.9) 4 (25.0) |
12 (48.0) 72 (66.1) 4 (50.0) |
0.189* |
|
Duration of work in the current healthcare facility (years) ≤5 (n=81) 6-10 (n=38) >10 (n=23) |
37 (45.7) 14 (36.8) 3 (13.0) |
44(54.3) 24 (63.2) 20 (87.0) |
0.017* |
|
Typical number of working days/week ≤4 (n=10) 5 (n=114) >5 (n=18) |
2 (20.0) 48 (42.1) 4 (22.2) |
8 (80.0) 66 (57.9) 14 (77.8) |
0.129* |
|
Duration of annual vacation (weeks) ≤4 (n=98) >4 (n=44) |
28 (28.6) 26 (59.1) |
70 (71.4) 18 (40.9) |
0.001* |
|
On call duties No (n=36) Yes (n=106) |
10 (27.8) 44 (41.5) |
26 (72.2) 62 (58.5) |
0.143* |
*Chi-square test, °Independent two samples t-test, SD: standard deviation
Low personal accomplishment
The age of participants who had low PA was significantly lower than that of those with high/medium PA (35.1±6.6 versus 38.2±10.8), p=0.035. Saudi participants were more likely than non-Saudis to have low PA (71.3% versus 53.2%), p=0.027. None of the participants who work ≤4 days/week compared to 68.4% and 66.7% of those who work 5 days or more/week, respectively, p<0.001. Participants who had shorter annual vacations (≤4 weeks) were more likely than those with longer vacations (>4 weeks) to report low PA (71.4% versus 45.5%), p=0.003. Participants with on-call duties were more likely than their peers to report low PA (73.6% versus 33.3%), p<0.001. Other studied sociodemographic and work-related factors were not significantly associated with low PA (Table 4).
|
Table 4: Factors associated with low personal accomplishment among the study participants (n=142) |
|||
|
Personal accomplishment |
p-value |
||
|
High/medium (n=52) N (%) |
Low (n=90) N (%) |
||
|
Gender Male (n=78) Female (n=64) |
30 (38.5) 22 (34.4) |
48 (61.5) 42 (65.6) |
0.615* |
|
Age in years Mean ± SD |
38.2±10.8 |
35.1±6.6 |
0.035° |
|
Marital status Single (n=34) Married (n=100) Divorced/widowed (n=8) |
8 (23.5) 42 (42.0) 2 (25.0) |
26 (76.5) 58 (58.0) 6 (75.0) |
0.121* |
|
Nationality Saudi (n=80) Non-Saudi (n=62) |
23 (28.7) 29 (46.8) |
57 (71.3) 33 (53.2) |
0.027* |
|
Job title Physician (n=25) Nurse (n=109) Others (n=8) |
10 (40.0) 38 (34.9) 4 (50.0) |
15 (60.0) 71 (65.1) 4 (50.0) |
0.642* |
|
Duration of work in the current healthcare facility (years) ≤5 (n=81) 6-10 (n=38) >10 (n=23) |
33 (40.7) 12 (31.6) 7 (30.4) |
48 (59.3) 26 (68.4) 16 (69.6) |
0.500* |
|
Typical number of working days/week ≤4 (n=10) 5 (n=114) >5 (n=18) |
10 (100) 36 (31.6) 6 (33.3) |
0 (0.0) 78 (68.4) 12 (66.7) |
<0.001* |
|
Duration of annual vacation (weeks) ≤4 (n=98) >4 (n=44) |
28 (28.6) 24 (54.5) |
70 (71.4) 20 (45.5) |
0.003* |
|
On call duties No (n=36) Yes (n=106) |
24 (66.7) 28 (26.4) |
12 (33.3) 78 (73.6) |
<0.001* |
*Chi-square test, °Independent two samples t-test, SD: standard deviation
Burnout
Most of divorced/widowed participants (75%) had burnout compared to 23.5% and 20% of single and married participants, respectively; p=0.002. Participants who had shorter annual vacations (≤4 weeks) were more likely than those with longer vacations (>4 weeks) to report burnout (28.6% versus 13.6%), p=0.045. Other studied sociodemographic and work-related factors were not significantly associated with burnout (Table 5).
|
Table 5: Factors associated with burnout among the study participants (n=142) |
|||
|
Burnout |
p-value |
||
|
No (n=108) N (%) |
Yes (n=34) N (%) |
||
|
Gender Male (n=78) Female (n=64) |
64 (82.1) 44 (68.7) |
14 (17.9) 20 (31.3) |
0.065* |
|
Age (years) Mean ± SD |
36.5 ± 9.2 |
35.1 ± 5.8 |
0.398° |
|
Marital status Single (n=34) Married (n=100) Divorced/widowed (n=8) |
26 (76.5) 80 (80.0) 2 (25.0) |
8(23.5) 20 (20.0) 6 (75.0) |
0.002* |
|
Nationality Saudi (n=80) Non-Saudi (n=62) |
61 (76.3) 47 (75.8) |
19 (23.8) 15 (24.2) |
0.951* |
|
Job title Physician (n=25) Nurse (n=109) Others* (n=8) |
20 (80.0) 82 (75.2) 6 (75.0) |
5 (20.0) 27 (24.8) 2 (25.0) |
0.878* |
|
Duration of work in the current healthcare facility (years) ≤5 (n=81) 6-10 (n=38) >10 (n=23) |
63 (77.8) 28 (73.7) 17 (73.9) |
18 (22.2) 10 (26.3) 6 (26.1) |
0.858* |
|
Typical number of working days/week ≤4 (n=10) 5 (n=114) >5 (n=18) |
10 (100) 84 (73.7) 14 (77.8) |
0 (0.0) 30 (26.3) 4 (22.2) |
0.171* |
|
Duration of annual vacation (weeks) ≤4 (n=98) >4 (n=44) |
70 (71.4) 38 (86.4) |
28 (28.6) 6 (13.6) |
0.045* |
|
On call duties No (n=36) Yes (n=106) |
24 (66.7) 84 (79.2) |
12 (33.3) 22 (20.8) |
0.127* |
*Chi-square test, °Independent two samples t-test, SD: standard deviation
Multivariate logistic regression analysis revealed that divorced/widowed participants were at a significantly higher risk of burnout compared to singles (AOR=18.92; 95%CI: 2.63-136.14), p=0.004. Compared to participants with short annual vacations (≤4 weeks), those with long annual vacations (>4 weeks) were at lower risk for burnout (AOR=0.27; 95% CI: 0.08-0.84), p=0.024 (Table 6).
|
Table 6: Binary logistic regression analysis for predictors of burnout among the study participants (n=142) |
|||||
|
B |
SE |
AOR |
95% CI |
p-value |
|
|
Marital status Singlea Married Divorced/widowed |
0.042 2.940 |
0.488 1.007 |
1.0 1.04 18.92 |
--- 0.40-2.71 2.63-136.14 |
0.931 0.004 |
|
Duration of annual vacation (weeks) ≤4a >4 |
-1.324 |
0.585 |
1.0 0.27 |
--- 0.08-0.84 |
0.024 |
a: Reference category, B: Slop, SE: Standard error, AOR: Adjusted odds ratio, CI: Confidence interval
Discussion
Palliative care is a medical specialty characterized by persistent stress, so people working in this field are subjected to continuous psychological morbidity and, consequently, burnout (16). This study explored the rate and determinants of burnout among palliative care health workers in one healthcare facility in Riyadh, Saudi Arabia.
Prevalence of burnout
In the current study, the prevalence of high EE was 49.3% whereas those of high DP and low PA were 62% and 63.4%, respectively, and the overall prevalence of burnout among palliative care health workers was 23.9%, with no significant difference between physicians, nurses, and others, while for physicians specifically, the rates of high EE, high DP, and low PA were 40%, 48%, and 60%, respectively, whereas the overall rate of burnout (high EE, high DP, and low PA) was 20%. In another Saudi study carried out among palliative care physicians, the prevalence of high EE, high DP, and low PE was 18.2%, 25%, and 25%, respectively (16). In Canada, the prevalence rates of high EE, high DP, and low PA were 36.4%, 15.1%, and 7.9%, respectively; with an overall rate of 38.2% (high EE or high DP) among physicians working at the palliative care department (18). In the United States, the prevalence of burnout among palliative care physicians ranged between 33% and 38.7% (19-21). In Singapore and Australia, rates of 41.9% and 24% have been reported (9, 22), respectively while in France, the rates of high EE and high DP were 9 and 4%, respectively among palliative care physicians (23). Also, in France (2016), the prevalence rates of high EE, high DP, and low PA were 9%, 4%, and 18%, respectively (23). In the Czech Republic, the prevalence of burnout among healthcare workers caring for patients in hospices was low (6%) (24).
In a recently published systematic review including 59 studies published between 2008 and 2020, the prevalence of burnout among healthcare workers in palliative care ranged between 3 and 66%; with no significant difference between physicians and nurses (15). Another systematic review and meta-analysis study conducted among palliative care nurses revealed that the pooled prevalence of EE was 24%, DP was 30%, and low PA was 28% (14). Also, in New Zealand, the prevalence of high burnout scores among nurses working in palliative care was 26.8% (25). In another systematic review conducted to assess the prevalence of burnout among health professionals (nurses, physicians, and social workers) working in palliative care, the prevalence of burnout was 17.3%, with nurses having higher levels of EE (19.5%) and DP (8.2%), while physicians had the highest level of low PA (41.2%). The highest prevalence of burnout was observed among those concerned with home care (19.6%) (2).
Apparent variation between different studies including, the present one, in the rates of overall burnout and its dimensions could be explained by the difference in demographic and work-related characteristics between studies as well as in the definition, cut-off, and using the tool in defining burnout (20, 21).
Factors associated with burnout
In the present study and after controlling confounders in multivariate logistic regression analysis, burnout was associated with participants` marital status as divorced/widowed healthcare workers were more likely than others to have burnout. In addition, healthcare workers with shorter annual vacations were more likely to express burnout than those with relatively longer annual vacations. In another Saudi study recently conducted among palliative care physicians, significant associates with burnout were job title, availability of some administrative departments, supporting health care staff, and pain relief medications. A systematic review included 59 studies that revealed that workers in general facilities had more significant burnout than those working in specialized facilities (15). In Canada (2020), older physicians (aged over 60) were associated with lower burnout (18). Among palliative care nurses, the commonest predictors of burnout were occupational factors followed by psychological factors (14). In France, physicians working on a palliative care mobile team were more likely to have high EE than their peers (23). In the Czech Republic, burnout was not associated with demographic factors, duration of experience, or type of hospice care (24).
Parola et al (2017) conducted a systematic review aimed at comparing the impact of the working environment in palliative care settings with other settings, on burnout among healthcare workers and observed that working in palliative care units or hospices was associated with lower levels of EE and DP, as well as higher levels of PA, compared with working in other settings (13).
The differences between the various studies, as regards the associated factors with burnout, could reflect their differences in demographic and cultural characteristics.
Limitations of the present study include the fact that it is a single-centre study, which could impact the ability to generalize its findings over other centres. The cross-section approach is considered a limitation as it proves association and not causality. Despite those limitations, the study has some strengths, including the high response rate, separating healthcare workers according to their job title to compare burnout between them, and using a valid tool to assess burnout. Further nationwide study including healthcare workers involved in palliative care from various regions of the Kingdom of Saudi Arabia is warranted to have a comprehensive image of the situation.
Conclusion
Burnout is a prevalent problem among healthcare workers working in palliative care in Riyadh, with no difference between physicians, nurses, and other workers. Divorced/widowed participants and those with shorter annual vacations were more likely to express burnout compared to their counterparts. Decision makers should take care of the working environment of this category of healthcare, particularly their annual vacation length, and specific attention should be given to divorced/widowed workers to reduce the burden of burnout among them.
Disclosures
Author Contributions
All authors have reviewed the final version to be published and agreed to be accountable for all aspects of the work.
Ethics Statement
An informed consent was provided by the patient to include the data anonymously. Furthermore, the institute where the case was reported from approved the publication of the case.
Data Availability
All data is provided within the manuscript.
Conflict of interest
The authors declare no competing interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Acknowledgements
Not Applicable