Volume 4, Issue 4
April 2024
Ultrasound Evaluation of Congenital Hip Dislocation and Other Parameters in Children
Ali N. Alshahablah, Qurain T. Alshammari, Haney A. Alsleem, Elgeili Yousif, Bushra H. Abdelmalik
DOI: http://dx.doi.org/10.52533/JOHS.2024.40404
Keywords: congenital hip dysplasia, ultrasound imaging, screening
Introduction: Congenital hip dislocation is caused by a wide spectrum of reasons, leading to disability among children. Many factors contribute to the disorder, including breech presentation, consanguineous marriage, and the hormone (Relaxin) which can promote ligament laxity in some patients with congenital hip dislocation. Additionally, being a firstborn child is said to increase the risk of developing the condition. The preferred method for assessing the hip in infants under 6 months of age is ultrasound (US). The Graf method is widely utilized among the various US screening techniques for the hip joint in this age group. The purpose of the study was to demonstrate the importance of ultrasonic imaging as a screening and diagnostic tool for congenital hip dislocation (CHD).
Methodology: The Hail Maternity and Childcare Hospital research was a retrospective descriptive study. A high-frequency transducer linear probe from GE Company was used for this study. Over the past two years (2020/2021), a total of 374 newborns were included in the study at the Hail Maternity and Childcare Hospital.
Results: At day five, 59.6% of the infants had a mean birth weight of 2.83±0.34 kg. Among the deliveries, 43.6% were conducted through caesarean section (CS), while 56.4% were spontaneous vaginal deliveries (SVD). There was a high percentage of females 51.1% than males 48.9%, The prevalence of CHD was 1.9%, with only seven children affected. Among these cases, three were females and four were males. Six affected children were delivered via CS, and one via SVD, and all had a breech presentation.
Conclusion: The occurrence of the disease was closely associated with the delivery method and presentation, but not influenced by age or gender, which contradicts previous research findings.
Introduction
Congenital hip dislocation (CHD), also known as developmental dysplasia of the hip (DDH), encompasses a wide range of manifestations, including subluxation, complete dislocation, and, in severe cases, joint bone dysplasia [1, 2]. Most patients are identified at birth through the presence of a click sign, which should be assessed by a pediatric specialist [3]. If not detected at birth, the abnormality may be recognized through the limping sign when the child begins to walk. Additionally, it is one of the primary causes of disability in children [4, 5]. The condition affects females more than males, with a ratio of 1:8 (M: F). In 35.2% of patients, both hips are involved, but the left side appears to be more commonly affected (37.6% vs. 27.2%) [4-7].
During a physical examination, a dislocated hip is characterized by limited abduction, leg length disparity, and asymmetry of the thigh or buttock fold [5]. If the diagnosis is delayed clinically, surgical intervention becomes necessary for the patients [5]. Ultrasonography (USG) is the preferred modality for evaluating the hip in newborns aged below six months. Among the various ultrasound imaging techniques for screening the hip joint, the Graf method is widely employed [4-7]. USG screening can be beneficial as the sensitivity can reach up to 88.5% [8]. Therefore, the utilization of US in diagnosis and screening has been widely done.
When evaluating CHD, the Graf method categorizes hip maturation and angles, offering several variations to choose from. Type I corresponds to a fully developed hip with an angle exceeding 60°. Two subtypes, Type Ia and Type Ib, are defined based on the angle, with Type Ia having an angle greater than 55° [4]. Type IIa is used to define an immature hip before 12 weeks of age and between the ages of 50 and 59, while Type IIb (acetabular dysplasia) is assigned to an immature hip after 12 weeks of age [4]. When the angle falls between 43 and 49 degrees, it is classified as Type IIc, which is further divided into Type IIc stable and Type IIc unstable. Type IId hip dislocations have an angle ranging from 43 to 49 degrees, with an angle greater than 77 degrees. Both Type III and Type IV hips exhibit a decentered position [4].
Radiological follow-up is necessary for every hip that has been treated once. Patients with positive ultrasound results should also be monitored after 4 to 6 weeks to assess their progress [6]. Newborns, especially those who are female or have risk factors, should undergo USG screening regardless of their clinical evaluation. The use of USG for early screening and diagnosis of DDH/CHD is a topic of debate, and further data is required. In infants below six months of age, it may still be the optimal choice, especially in cases where the clinical examination is inconclusive [5, 6]. There is currently no international consensus regarding the use of ultrasound as a screening method for DDH/CHD. The question of whether all infants should undergo universal screening ultrasound or only those with risk factors or clinical hip instability should undergo selective screening remains unresolved. Moreover, the optimal timing for performing an ultrasound examination is still unknown [7]. The American College of Radiology also recommends conducting a conventional ultrasonography examination in the transverse view with the hip flexed at 90° if there are changes in the connection between the posterior acetabulum and the femoral head under gentle load, indicating hip instability [5].
The measurement technique utilizes three anatomic landmarks (the iliac line, triradiate cartilage, and labrum) to determine the angles. The maximum angle is defined as the angle formed between the acetabular roof and the vertical cortex of the ilium in the coronal plane. An angle less than 60° indicates a shallow acetabulum. The Graf angle is obtained by drawing a vertical line through the ilium. This angle is crucial in the sonographic Graf categorization method [4-7]. Our research objective was to study CHD in newborns and highlight the role of ultrasound imaging technology as screening and diagnostic imaging for CHD. Specifically, this study aims to calculate the gender distribution, mean birth weight, and mean age (in weeks) for babies, to estimate the prevalence of CHD and to measure the association between the disease and gender, mode of delivery, and presentation of the baby.
Methods
Study design and data collection
A retrospective descriptive study was conducted at the Maternity and Childcare Hospital (MCH) in Hail, Saudi Arabia to study CHD in newborn babies and highlight the role of ultrasound imaging technology as screening and diagnostic imaging for CHD. Data on livebirths between 2020 and 2021 was recalled from electronic medical records and retrospectively reviewed. Data collection sheet included CHD diagnosis, maternal and infant age at the time of study, type of birth, mode of delivery, presentation of the baby, and ultrasonography findings. Confidentiality of the patients was maintained. Approval for this research was received from the Institutional Review Board of the University of Hail with approval number: H-2022-087.
Study settings and patients
The study population included all livebirths who were delivered in Hail MCH between 2020 and 2021. The requirement for informed consent was waived because of the retrospective nature of the study. Stillborn babies and infants with incomplete medical records were excluded from the study.
The sample size formula,
n=(Z²p(1-p))/d²
was used to calculate the sample size, where n denotes the sample size at a 95% confidence level, Z=1.96, P denotes the population proportion and d denotes the margin of error. Overall, out of 13200 livebirths between 2020-2021, 374 babies were selected for the study via systematic random selection sampling.
Procedures
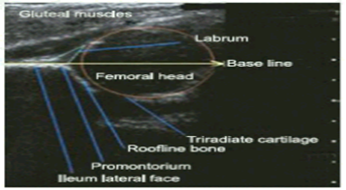
Patient preparation: The infant was dressed in comfortable clothes prior to examination. During examination, the baby was positioned in the lateral decubitus position, with the hips slightly flexed, adducted, and medially rotated (Figure 1). Subsequently, a high-resolution linear transducer was used to obtain a coronal sonogram. A special gel was applied to the area, the special gel is water-based; so, it should not leave marks on the clothes or skin, also the sound waves could travel properly. After the exam, ultrasound gel was cleaned.
Technique: The examination was conducted using the Graf method on an ultrasound scanner. The hip was assessed by measuring two angles created by three lines drawn from three specific points: the lateral edge of the acetabulum, the bottom of the acetabulum, and the acetabular labrum. These lines include the bony roof line, the baseline, and the cartilage roof line, all measured at the acetabular labrum (Figure 1). Once these lines were drawn, the bony roof angle (referred to as the alpha [α] angle) and the cartilage roof angle (known as the beta [β] angle) were determined (Figure 2).
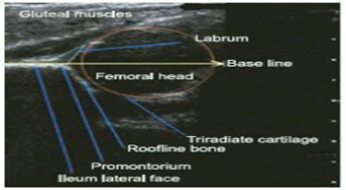
Figure 1: Infant hip joint components seen on US.
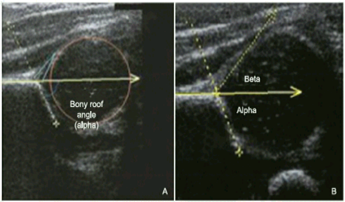
Figure 2: Quantifying Roof Angles in Skeletal and Cartilaginous Structures: α and β Measurements. A Measurement of the bony roof angle (α) angle, B Measurement of the cartilage roof angle (β) angle.
Statistical analysis
The Statistical Package for Social Science (SPSS, version 26, IBM Corp., Chicago, Il, USA) was utilized for all analyses and calculations. To assess the normality of continuous variables, the Kolmogorov-Smirnov test was employed. Continuous variables were presented as means ± standard deviations, while categorical variables were presented as proportions. A comparison between the two groups for quantitative variables was conducted using an independent sample t-test, while the chi-square test was used for categorical variables. The results were displayed in tables and pie charts. Furthermore, a binary logistic regression analysis was conducted to identify the factors associated with congenital hip dislocation. The odds ratio (OR) and confidence interval (95% CI) were reported. Statistical significance was considered for p-values less than 0.05.
Results
This study included 374 newborn babies with a higher proportion of females (51.1%) than males (48.9%) and the mean weight of the babies was 2.83±0.34 whereas the mean maternal age was 29.84±6.60. Only 7 (1.9%) of the babies had congenital hip dislocation (Figure 3). The majority 99 (25.0%) of mothers had 2 deliveries and most of them had a spontaneous vaginal delivery 211 (56.4%) as compared to the caesarean section 163 (43.6%) whereas 250 (66.8%) of the babies had a cephalic presentation and 124 (33.2%) had a breech presentation (Table 1).
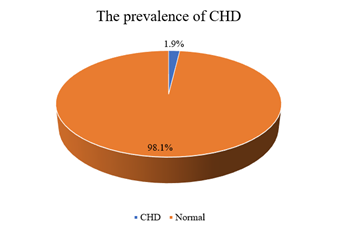
Figure 3: Prevalence of CHD.
|
Table 1. Background characteristics of the participants included in the study |
||
|
Variables |
Scale |
Total = 374 n (%), Mean ± SD |
|
Gender |
Female |
191 (51.1) |
|
Male |
183 (48.9) |
|
|
Weight of the baby (kg) |
2.83±0.34 |
|
|
Maternal age (years) |
29.84±6.60 |
|
|
CHD |
CHD |
7(1.9) |
|
Normal |
367(98.1) |
|
|
Number of deliveries |
0 |
55 (14.7) |
|
1 |
71 (19.0) |
|
|
2 |
96 (25.0) |
|
|
3 |
66 (17.6) |
|
|
4 |
51 (13.6) |
|
|
5 |
30 (8.0) |
|
|
6 |
5 (1.3) |
|
|
Mode of delivery |
CS |
163 (43.6) |
|
SVD |
211 (56.4) |
|
|
Baby Presentation |
Breech |
124 (33.2) |
|
Cephalic |
250 (66.8) |
|
CHD: Congenital hip Dislocation; CS: Caesarean section; SVD: Spontaneous vaginal delivery
A comparison of children with and without CHD showed that 7 (5.6%) of the children with CHD had breach presentation and 117 (94.4%) were normal with breach presentation. There was significance in both groups for the presentation of the baby (p=0.001) whereas there was no significant difference found in both groups for maternal age, gender of the baby, mode of delivery, No. of deliveries and presentation of babies (p>0.05) (Table 2).
|
Table 2. Comparison of congenital hip dislocation scores with participants’ background characteristics |
||||
|
Variables |
Scale |
CHD |
P-value |
|
|
CHD n (%) |
Normal n (%) |
|||
|
Maternal age |
32.43±6.29 |
29.79±6.61 |
0.296 |
|
|
2.84±0.33 |
2.83±0.34 |
0.957 |
||
|
Gender |
Male |
3 (1.6) |
180 (98.4) |
0.746 |
|
Female |
4 (2.1) |
187 (97.9) |
||
|
Mode of delivery |
CS |
6 (3.7) |
155 (96.3) |
0.071 |
|
SVD |
1 (0.5) |
210 (99.5) |
||
|
No. of delivery |
0 |
1 (1.8) |
54 (98.2) |
0.273 |
|
1 |
0 (0.0) |
71 (100) |
||
|
2 |
2 (2.1) |
94 (97.9) |
||
|
3 |
0 (0.0) |
66 (100) |
||
|
4 |
3 (5.9) |
48 (94.1) |
||
|
5 |
1 (3.3) |
29 (96.7) |
||
|
6 |
0 (0.0) |
5 (100) |
||
|
Presentation of baby |
Breech |
7 (5.6) |
117 (94.4) |
0.001 |
|
Cephalic |
0 (0.0) |
250 (100) |
||
A binary logistic regression analysis was performed to find the associated factors of CHD. Results showed that all variables were independent predictors of congenital hip dislocation and there was no signification relationship found between congenital hip dislocation and variables (Table 3).
|
Table 3. Logistic regression analysis on participants’ socio-demographic characteristics with the prevalence of congenital hip dislocation |
||||
|
Variables |
Scale |
OR |
(95% CI) |
P-value |
|
Age |
0.995 |
(0.877-1.129) |
0.941 |
|
|
Weight |
1.136 |
(0.094-13.778) |
0.920 |
|
|
Gender |
Male |
1.082 |
(0.200-5.854) |
0.927 |
Discussion
A retrospective descriptive cross-sectional study was conducted to investigate CHD in all live births and emphasize the role of ultrasound imaging as a screening and diagnostic tool for CHD. Data was collected using a specific form that included information on the health of the infant and the mother. The study found that the average maternal age was 29.65 years, ranging from 19 to 41 years. The prevalence of CHD was 1.9%, with only seven children out of 367 diagnosed with the condition. The incidence rate of CHD was calculated to be 3.5 per 1000 live births in the study conducted at Aseer Central Hospital [9]. Moreover, additional studies demonstrated that among the patients referred, 80% and 20% had normal stable hips, respectively [6].
Regarding gender distribution, there were 3 (1.6%) females and 4 (2.1%) males. The Aseer Central Hospital study reported a male-to-female ratio was 1:3.6, and also noted that Saudis accounted for 97.7% (n = 292) of the population [9]. Similarly, a retrospective study conducted by Omar Al Mohrej at a Tertiary Hospital in Riyadh, Saudi Arabia, identified a total of 176 patients diagnosed with CHD, of which 151 were female (85.8%) [10]. In our study, 3 out of the 7 cases were seen in fifth-born children, whereas 1 case each was seen in a firstborn and sixth-born. The birth order of the newborns with DDH/CHD ranged from 1 to 6. In the Aseer study, first-born children constituted 216 (25.9%) of the population.
This study utilized a high-frequency transducer linear probe from GE Company in order to arrive at at radiological diagnosis of DDH/CHD among newborn children. In contrast, in the Al Mohrej et al. study, plain x-ray of pelvis was taken to confirm the diagnosis of DDH/CHD at the age of three months [10]. The initial screening clinical examination for the condition in children was performed between the ages of three and six days, with an average age of five days. In the Aseer study also, plain x-ray of pelvis was taken to confirm the diagnosis of DDH/CHD at the age of three months. Over 32% (n = 96) of patients were diagnosed within the first six months of life, with an average age at diagnosis ranging from 14.5 to 19.7 months [9]. Today, however, ultrasonography (USG) is the preferred modality for evaluating the hip in newborns and infants aged below six months [11, 12]. Compared to standard radiographs, the US allows dynamic evaluation to determine the presence of instability in addition to the dysplasia. It dramatically improves the sensitivity for hip dislocation diagnosis. The universal USG screening observed DDH/CHD in a number of children with normal clinical examinations and absence of risk factors, according to a recent retrospective study [13]. The American College of Radiology also recommends conducting a conventional USG examination in the transverse view with the hip flexed at 90° if there are changes in the connection between the posterior acetabulum and the femoral head under gentle load, indicating hip instability [4]. Radiological follow-up is necessary for every hip that has been treated once. Patients with positive USG results should also be monitored after 4 to 6 weeks to assess their progress [5]. Newborns, especially those who are female or have risk factors, should undergo USG screening regardless of their clinical evaluation.
With regard to the mode of delivery, in our study, 211 babies were delivered via SVD out of which 1 was diagnosed with DDH/CHD, whereas 161 babies were delivered via CS among which 6 cases of DDH/CHD were identified. All of the 7 (5.6%) affected newborns had a breech presentation. Likewise, in the Aseer Hospital study, 268 (89.3%) deliveries were SVD, 28 cases (9.3%) were CS, and 10% were breech deliveries in 29 cases [9]. Breech presentation was found to be a risk factor in 17.3% of patients in the systematic review by Sadat-Ali et al. [4].
DDH/CHD is a prevalent pediatric orthopedic condition with a significant occurrence rate. As mentioned earlier, timely detection is crucial to minimize the need for surgical interventions, which often come with high complication rates, as evidenced by existing research. Consequently, the establishment of a national screening program for early DDH detection is strongly recommended.
Such a comprehensive DDH/CHD screening program should begin with a thorough review of the patient's medical history to identify relevant risk factors, allowing for the categorization of individuals into high-risk and low-risk groups. Subsequently, a meticulous physical examination using well-established techniques for DDH/CHD detection should be conducted. A 2017 study by Kang RY, et al. [5] on DDH/CHD at Dongguk University's Faculty of Medicine's Department of Radiology in Korea recommended that all infants undergo a clinical assessment of their hips shortly after birth. According to current published criteria, this assessment should be performed at each planned well child check until the age of one year. If a child exhibits intermediate findings or has elevated risk factors during a routine examination, US imaging should be conducted between 3 and 6 weeks of age, depending on the specific risk factors. USG is a well-established radiological method for early DDH/CHD identification, characterized by its safety, cost-effectiveness, and widespread availability. Alternatively, if reliable US is not available, plain radiographs should be taken between 4 and 5 months of age [4].
Expanding our perspective, it becomes apparent that a comprehensive DDH/CHD screening program should encompass more than just clinical and radiological aspects. It should take a holistic approach, incorporating risk factor assessment, evaluation of radiological parameters, and engagement with the patient's family. This comprehensive approach is essential for gaining a nuanced understanding of DDH/CHD patterns in the Saudi Arabian context and for making comparisons with regional and global data.
In our analysis, we focused on a selected set of socio-demographic characteristics derived retrospectively from electronic medical records. These included age, weight, and gender, as potential predictors of DDH/CHD. This was a grave study limitation. While these variables are important factors to consider in understanding the prevalence of DDH/CHD, it is essential to acknowledge that there may be other influential factors that were not included in this analysis due to data limitations. The selection of these socio-demographic characteristics was based on available data within our electronic medical records, and we recognize that a comprehensive understanding of DDH/CHD incidence may require a more extensive set of variables, including clinical and genetic factors. Future research endeavors could benefit from the inclusion of additional predictors, which may provide a more nuanced perspective on the determinants of DDH/CHD. Other study limitations include the sample size which was relatively small, directly impacting the statistical power and precision of the results. Further, due to the unavailability of follow-up data, the progression of the condition and the effectiveness of the intervention cannot be evaluated. Additionally, the study was conducted at a single center, which limits the generalizability to other populations or on the community. A multicenter approach or collaboration with other institutions may allow for the exploration of a broader range of variables and potentially enhance the generalizability of findings. Our study represents an initial exploration of the relationship between socio-demographic factors and DDH/CHD, and further research is needed to validate the results in larger and more diverse populations.
Conclusion
This retrospective descriptive study aimed to investigate congenital hip dysplasia (CHD) in newborns and the role of ultrasound imaging as a screening and diagnostic tool. The study found a prevalence of 1.9% for CHD among the study population, with a higher proportion of females affected. The mean ages of the infant and the mother were 5 days and 29.65 years respectively. No association was found between gender (p = 0.7) and CHD, but the condition was strongly associated with the presentation at birth (p = 0.001) and the mode of delivery (p = 0.05). The study emphasized the importance of early detection and diagnosis of CHD to prevent delayed treatment and associated complications.
Disclosure
Declaration
The authors declare no conflict of interest.
Funding
None
Ethical Considerations
The study has been approved by the institutional review board of the University of Hail with approval number: H-2022-087.
Data Availability
All data is available within the manuscript, and the survey is attached as a supplementary material.
Author Contribution
All authors contributed equally in the conceptualization, data collection, data analysis and writing of the paper.