Volume 3, Issue 12
December 2023
Imaging of Kidney Stones: CT Urography, Ultrasound, and Stone Composition Analysis
Marwah Fallatah, Rafaa Jaafari, Aryaf Alshammari, Abdulrahman Bashaikh, Israa Alshehri, Hassan AlSubaie, Mooza Alabbasi, Ali Aldayin, Abdullah Al Rasheed, Ahmed Khayat, Hamza Tolah
DOI: http://dx.doi.org/10.52533/JOHS.2023.31206
Keywords: Kidney Stones, CT Urography, Ultrasound, Stone Composition, Dual Energy CT (DECT)
Kidney stone disease, prevalent since ancient times, affects around 12% of the global population, with a higher incidence in males. Recurrence is common, and the formation of stones is influenced by genetic, metabolic, environmental, and structural factors. Ultrasonography, as the initial diagnostic tool, is non-invasive and radiation-free, making it suitable for initial evaluations. However, for more precise diagnosis, especially in complex cases, CT scans, including Dual Energy CT (DECT), are preferred due to their higher accuracy. This review also delves into the historical evolution of diagnostic methods, from the once-popular Intravenous Urography (IVU) to the advanced DECT, which offers detailed insights into stone composition. While each imaging modality has its advantages and limitations, CT scans remain the gold standard for their comprehensive analysis capability. The choice of imaging technique is influenced by factors such as stone size, patient characteristics, and clinical context. This review underscores the importance of personalized strategies in selecting the most suitable imaging modality for effective diagnosis and management of kidney stone disease.
Introduction
Kidney stone disease, also recognized as nephrolithiasis or urolithiasis, has a documented history tracing back to ancient Egyptian times, approximately 2000 years ago. This condition is a prevalent health issue, with statistical analyses suggesting that around 12% of individuals worldwide are likely to encounter urinary stones at some point in their lifetime (1, 2). Notably, there is a gender disparity in the incidence of this disease, with males being more susceptible than females. A significant aspect of this condition is its tendency to recur; about half of the individuals who have been diagnosed with kidney stones will likely face a recurrence within ten years following their initial diagnosis.
Kidney stones typically form in the renal calyces and pelvis. The exact mechanisms leading to the formation of these stones remain somewhat unclear. However, the predominant theory is that they result from the accumulation of minerals on a mucoprotein matrix, which acts as a nidus, or focal point, for stone development. This process of mineral deposition is complex and influenced by various physiological factors (3).
Several risk factors have been identified for the development of kidney stones. These include genetic predispositions (4, 5), with a notable correlation to family history, suggesting a hereditary component to the disease. Metabolic syndrome, a cluster of conditions including high blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol levels, also plays a significant role (6-8). Environmental factors, such as residing in hot climates, contribute to the risk by promoting dehydration, a known catalyst for stone formation. Chronic dehydration, irrespective of climate, is another crucial risk factor. Abnormalities in the urinary tract structure or function can predispose individuals to stone formation. Additionally, recurrent urinary tract infections are also recognized as a significant contributing factor to the development of kidney stones.
In terms of diagnostic approaches, ultrasonography (US) is often the initial imaging method employed for the detection of urinary stones. It is a preferred choice due to its non-invasive nature, absence of radiation exposure, and general effectiveness in identifying stones. However, in cases where ultrasonography is insufficient, particularly when ureteric stones are suspected but not clearly identified, computed tomography (CT) scans are employed (9). In some instances, Dual Energy CT (DECT) provides an even more precise diagnostic tool. CT and DECT are considered the gold standard for their superior accuracy in detecting and characterizing urinary stones, especially in complex or ambiguous cases. These advanced imaging techniques offer critical insights, aiding in the effective diagnosis and subsequent management of renal stone disease.
Methodology
This study is based on a comprehensive literature search conducted on November 14, 2023, in the Medline and Cochrane databases, utilizing the medical topic headings (MeSH) and a combination of all available related terms, according to the database. To prevent missing any possible research, a manual search for publications was conducted through Google Scholar, using the reference lists of the previously listed papers as a starting point. We looked for valuable information in papers that discussed imaging of kidney stones, particularly CT urography, ultrasonography, and stone composition analysis. There were no restrictions on date, language, participant age, or type of publication.
Discussion
The urinary system, a pivotal component of human anatomy, comprises the kidneys, ureters, urinary bladder, and urethra. This system plays a crucial role in maintaining homeostasis by filtering blood, eliminating waste via urine, and managing various other physiological functions (10). The aging process significantly impacts the kidneys' functionality, notably reducing the glomerular filtration rate (GFR) and nephron count. This decline can be exacerbated by diseases leading to glomerulosclerosis and podocyte dysfunction, affecting urine production and excretion (11). The urethra, differing anatomically between males and females, completes the urinary system. In females, the urethra opens anterior to the vagina, while in males, it includes the prostatic, membranous, and spongy urethra (12). The urethral sphincters regulate urine flow, maintaining continence.
Urolithiasis often presents as acute renal colic, with severe, colicky pain due to urinary tract stone obstruction, varying in location based on the obstruction site. Aside from pain, symptoms can include dysuria, urinary frequency, urgency, nausea, vomiting, fever, and hematuria. Small stones might not cause obstruction but can lead to recurrent urinary tract infections (13, 14).
Diagnostic evaluation includes imaging, blood and urine tests to assess renal function, electrolyte levels, and the presence of infection. The white blood cell count may rise in response to stress or infection, while chronic calculus disease can lead to reduced hemoglobin levels. Urine analysis reveals hematuria, pyuria, and pH levels, aiding in the selection of appropriate antibiotics for infection management.
Imaging Modalities
Imaging plays a vital role in diagnosing, treating, and monitoring renal stone disease, offering insights into the urinary system's anatomy and function. Essential for confirming stones in patients with flank pain, it guides treatment decisions and surgical success predictions (15). Since 1930, urography has been the primary diagnostic tool for urinary disorders, peaking at 10 million urograms annually in the United States by 1980. This number has since dropped to under 600,000, largely due to advances in CT scanning and the US. CT's introduction in 1975 and the 1989 advent of spiral technology revolutionized urinary calculi and tract imaging. Today, a range of techniques including X-rays, ultrasound, and CT are used, each with distinct advantages. Selecting the best method depends on factors like stone size and location, patient characteristics, and clinical context. For a thorough examination of urinary stones, CT scans, particularly non-contrast CT, are generally preferred (16).
Ultrasonography (US)
The US is effective in detecting kidney stones regardless of their composition, identifying stones as small as 0.5 mm as bright spots with shadowing in the urinary tract. Ureteral stones often occur at the ureteropelvic junction, though many are found in the distal ureter. However, ultrasound's effectiveness is limited if the bladder is not full. Visualizing ureteral stones directly can be challenging due to intestinal gas and the ureter's deep position within the pelvis. In obese patients, ultrasound imaging can be hindered by excessive fat. Some studies suggest that higher renal resistive indexes in Doppler sonography might indicate an acute blockage, and asymmetric ureteral jets seen in color Doppler could point to a lower ureter stone, but these findings are inconsistent (17). The renal twinkling artifact, often linked to kidney stones, has a relatively low sensitivity of 55% in clinical settings (18). Ultrasound is accessible and cost-effective, but its diagnostic accuracy for kidney stones is limited, with a detection sensitivity of around 45% (19). While detection rates increase with the size of the stone, ultrasound's accuracy in measuring stone size is debatable, often overestimating due to unclear stone edges (20). Comparisons between ultrasound and CT show differences in measurements, with ultrasound typically giving larger estimates than CT, especially for stones smaller than 5 mm (21). Yet, a recent study indicates that when performed by experienced sonographers specializing in urological ultrasound, it can effectively detect stones and assess their size (22). Ultrasound can also identify secondary issues like blockages, infections, or abscesses. Its diagnostic sensitivity improves significantly when these secondary signs of obstructive uropathy are considered. Ultrasound is the preferred method for pregnant women and children, where minimal radiation is crucial, and is recommended for follow-up. A recent study advocates for an ultrasound-based follow-up for ureteral stones, significantly reducing radiation exposure, especially for patients with recurring renal colic (23).
Urography
Intravenous Urography (IVU), also known as intravenous pyelography, is an important diagnostic tool for identifying the presence, size, location, and obstruction caused by stones in the urinary tract. In this procedure, a contrast agent is injected into the patient's vein, which the kidneys then filter and excrete. This allows for X-ray images of the kidneys, ureters, and bladder to be taken at different intervals as the contrast moves through the urinary system (24). Historically, IVU has been widely used to examine the urinary tract, but its effectiveness in detecting urinary stones is less compared to other methods like CT scanning. IVU may miss smaller stones, especially those under 5 mm (3).
IVU is particularly useful for assessing obstructions caused by urinary stones. The contrast material highlights the urinary tract, aiding in identifying and detailing any blockages or narrowing in the ureter. Additionally, IVU can evaluate kidney function by observing how the contrast material is excreted, thereby indicating the health of the kidneys and the patency of the urinary system. This method helps to determine how urinary stones affect kidney recovery (25).
Despite its benefits, IVU has limitations. It uses ionizing radiation, which may restrict its use among certain groups, such as pregnant women and children. IVU primarily focuses on imaging and locating urinary stones, offering limited information about their composition. When considering IVU for studying urinary stones, it is important to weigh the potential risks associated with radiation exposure and its limited capabilities in stone characterization (26).
Computed tomography (CT)
CT scans are quick to perform and extremely effective in detecting stones of all sizes, with some studies showing nearly 100% sensitivity. Besides identifying stones, CT can assess how much the stone is blocking the urinary tract, map out the anatomy important for surgery, and spot other possible causes of pain, including conditions like appendicitis, endometriosis, hemorrhagic cysts, and ovarian torsion (9).
There are several types of CT scans used in the evaluation and management of urinary stones:
Unenhanced CT
Since its introduction in the late 1990s, unenhanced CT, particularly the CT KUB (kidneys, ureters, and bladder), has become the preferred diagnostic method for suspected urolithiasis, especially in emergency settings. Accounting for over 20% of CT exams for acute abdominal pain (27), these non-contrast scans are highly sensitive and specific (over 95%) in detecting urinary stones, capable of identifying stones as small as 1–2 mm in size, shape, and location. They are invaluable in diagnosing potential urinary stone issues, revealing obstruction signs like hydronephrosis or hydroureter, and identifying related conditions requiring medical attention. Modern equipment enables quick image acquisition, with the capability to customize examinations based on the known calculus location (28). These scans can detect 99% of renal tract calculi, which vary in density from calcium oxalate and phosphate stones (400–800 HU) to softer stones like uric acid and cystine (100–200 HU). Unique features like the "rim sign" aid in differentiating urinary calculi from other pathologies. Overall, non-contrast CT scans are an essential and effective tool in the investigation and management of urinary tract stones (3).
CT Intravenous Urography (CTU)
CTU, also known as CT intravenous pyelography (CT IVP), has become the preferred method for imaging the genitourinary tract, replacing the standard IVU. This technique involves injecting an iodine-based contrast agent intravenously to enhance the visibility of the urinary tract during the CT scan (29). CT IVU effectively localizes stones in the kidneys, ureters, or bladder by capturing images as the contrast agent moves through the urinary system. CTU is highly accurate, with a sensitivity of 96–100% and a specificity of 94–100% for detecting ureteric and bladder stones. It offers both anatomical and functional insights but comes with the trade-off of higher radiation exposure (30).
Dual Energy CT (DECT)
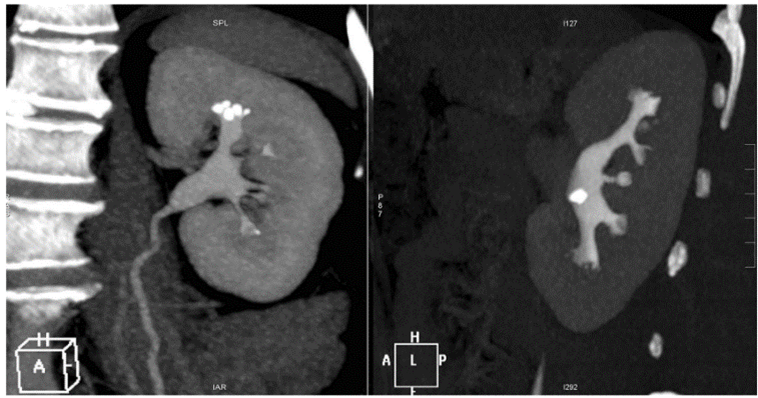
DECT is an advanced imaging technology specifically beneficial in studying urolithiasis, utilizing two X-ray tubes at different kilovoltage levels to produce various imaging datasets. Its core principles, including the X-ray tube’s power and the material properties affecting Compton and Photoelectric effects, are similar to traditional X-ray imaging (31). DECT leverages the concept that materials respond differently to varying X-ray photon energies, allowing for a unique energy-dependent attenuation profile for each material, measured in Hounsfield Units (HU). This attenuation, influenced by the material’s atomic number and electron density, varies inversely with the X-ray tube’s energy output. DECT's methodology, akin to CTU, involves multiple acquisition phases. Initially, an unenhanced scan of the abdomen and pelvis is performed. Then, patients receive intravenous furosemide to enhance the visibility of the urinary system, followed by various post-contrast phases that help in identifying different aspects of the urinary tract and potential abnormalities. DECT’s unique capability lies in its use of both low-energy and high-energy X-rays, allowing it to differentiate materials based on their atomic composition. This feature is particularly useful in identifying the types of urinary stones by evaluating their attenuation properties at different energy levels. DECT produces color-coded images, making it easier to distinguish between different stone compositions, such as calcium oxalate and uric acid stones (Figure 1) (9).

Figure 1: Dual-phase CT and urolithiasis. Visibility of stones (stone density 860 HU) within the collector system (density 280 HU) and renal parenchyma anatomy. (9)
Overall, DECT proves more effective than single-energy CT in differentiating stone types, particularly in discerning uric acid stones from others, and offers a color-coded representation of various stone components about their atomic composition. This technological advancement not only aids in the precise diagnosis of urolithiasis but also enhances the understanding of the stone’s composition, aiding in targeted treatment approaches.
Various types of urinary stones
The most common type of urinary stone is made of calcium oxalate (32). These stones are broadly classified into five types (33): calcium, magnesium ammonium phosphate, uric acid, cystine, and those related to medications and their byproducts. Calcium stones represent 70-80% of all urinary stones, with calcium oxalate stones being the most common, constituting 60% of all stones (34). Factors like hypercalciuria, which can be due to insufficient calcium reabsorption in the kidneys or increased calcium absorption in the intestines, lead to their formation. Other contributing factors include low citrate levels, high oxalate levels, and abnormal uric acid metabolism. Hyperoxaluria, which can be primary (due to a genetic disorder) or secondary (associated with other medical conditions or excessive vitamin C intake), is also a key factor in the formation of calcium stones (3).
Magnesium ammonium phosphate calculi (struvite stones)
Making up 15-20% of urinary stones, struvite stones are caused by urease-producing bacteria like Proteus and Pseudomonas (35). These bacteria increase urine pH, leading to the formation of large stones, often filling the kidney's collecting system and resembling a stag's antler.
Uric acid stones
Comprising 5-10% of urinary stones, uric acid stones are influenced by urine acidity and high levels of uric acid. Risk factors include gout, chronic diarrhea, obesity, and diabetes. These stones are typically not visible on standard radiography but can be detected using CT scans (36).
Cystine stones
Accounting for 1-3% of urinary stones, cystine stones arise from cystinuria, a genetic condition affecting renal transport. These stones often have a ground-glass appearance and may show low-attenuation areas on CT scans (3).
Medication-induced stones
Long-term or excessive use of certain medications can lead to medication-induced stones. Notable examples include indinavir, used for Human Immunodeficiency Virus (HIV) treatment, and some herbal supplements like ephedrine and guaifenesin. These stones might be radiolucent on CT scans. Diagnosis often involves considering the patient's medication history and symptoms. Treatment focuses on modifying medications, adjusting dosages, increasing fluid intake, and potentially altering urine pH (3).
Conclusion
Renal stone disease, causing acute pain, often starts with ultrasonography for diagnosis due to its non-invasiveness. However, CT scans are the gold standard, providing detailed information on the stone's presence and characteristics, essential for prognosis and treatment. DECT further excels in diagnosing renal stones, offering in-depth analysis of the stone's anatomy and composition, crucial for effective treatment and preventing relapses, making it a vital tool in managing this condition.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding
Ethical consideration
Non applicable
Data availability
Data that support the findings of this study are embedded within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.