Volume 1, Issue 4
July 2021
A Case of Successful Management of a Knotted Ureteral Stent in the Proximal Part of a JJ Stent
Bander Binjabaan, Abdullah Alfulaij, Ali Alabandi, Mutadah Alnemer
DOI: http://dx.doi.org/10.52533/JOHS.2021.1401
Keywords: ureteral stent, knotted stents, JJ stent, Proximal stenting, gentle traction, successful management
Ureteral stent usage is a routine practice in urology practice. They are usually safe, but complications may occur and are variable. They can be categorized into immediate, early and late complications. Stent knotting is a rare complication with less than 30 cases reported in the literature. We report a case of a 50-year-old man in which a complete knot was found in the proximal part of the JJ stent. The knotted stent was gently pulled and successfully removed under fluoroscopic guidance after failed attempts to use a guidewire as well as the use of a semi-rigid ureteroscopy. Gentle traction was used and resulted in complete removal of the stent without any complications. In conclusion, gentle traction of a knotted JJ stent of the proximal part is a successful method and can be used. However, careful planning and prediction of major injuries such as avulsion and kidney injury should be considered.
Introduction:
Ureteral stent (JJ stent) usage has become a routine practice used as a measure of temporary or permanent drainage of the occluded upper urinary tract (1). It was first described by Zimskind et al. in 1967 (2). With time, many improvements in ureteral stent design and composition material have taken place, resulting in the further improvement of stent quality. Stents are used to drain urine from kidney to bladder, and usually are safe. Complications can range from minor to major and are categorized into immediate, early or late complications. Minor complications may include hematuria, dysuria, frequency, flank and suprapubic pain, while major complications can include vesico-ureteric reflux, migration, encrustation, urinary infection, stent fracture, necrosis and ureteroarterial fistula (3). Knotting of the ureteral stent is uncommon and has been reported in less than 30 cases. Therefore, it can be considered a rare complication (4). Here, we report a case of a male patient that reported with a knotted JJ stent which was then removed successfully without any complications.
Case Report:
A 50-year-old man on warfarin and with a past history of laparotomy in 2020 due to mesenteric ischaemia causing bowel ischemia was referred to our urology clinic from a different hospital with a three-month history of a right proximal ureteric radiopaque stone about 8 mm in diameter. Initially, the patient complained from right flank pain and dysuria. His family history was insignificant, and he was non-smoker. Upon questioning, the patient reported that he had undergone a JJ stent insertion outside our hospital after three unsuccessful sessions of Extracorporeal Shock Wave Lithotripsy (ESWL). On examination, the patient was vitally stable while his abdominal examination revealed a local laparotomy scar, laxed and soft abdomen on palpation with no signs of tenderness and no palpable bladder. Lab investigation included complete blood count, liver function test, renal function test and urine analysis. All laboratory workup was normal except for urine analysis and his bleeding profile. His urine analysis showed pus, 20-50 red blood cells (normal range: ★ 2 RBCs/hpf) and leukocyte esterase while his blood profile reported high values likely due to his warfarin treatment. Afterwards, a urine culture was obtained, and no growth was reported. We moved forward with a right semi-rigid ureteroscope and laser lithotripsy with complete stone fragmentation and a right JJ stent 4.8 French (Fr) was inserted under fluoroscopic guidance. A kidney, ureter and bladder (KUB) x-ray requested by our department after the operation showed optimal placement and coiling of right ureteral stents (Figure 1).

Figure 1: Kidney ureter and bladder X-ray shows normal coiling of the JJ stent.
Removal of the right double-J stent by cystoscopy under spinal anesthesia was scheduled one month after the operation. On the day of the removal, there was difficulty when removing the right JJ stent. After straightening the distal coil, reaching the mid part of the urethra was difficult. A plain radiograph that was taken showed a knotted ureteral stent at the ureteropelvic junction (UPJ) (Figure 2).
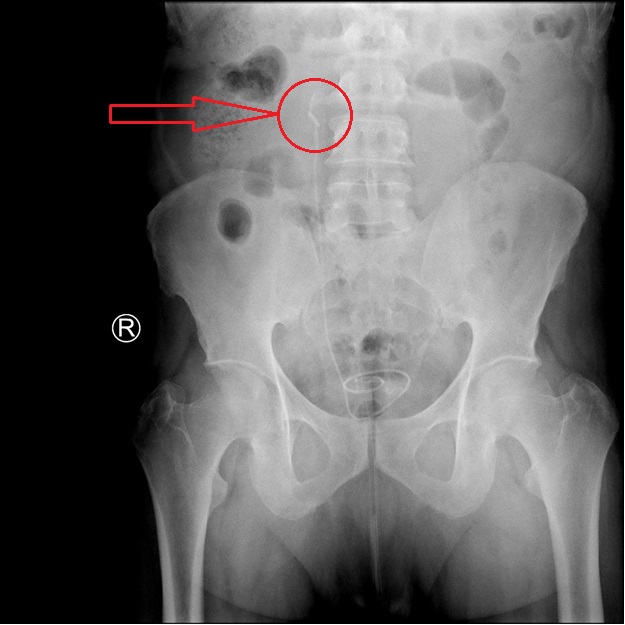
Figure 2: Kidney ureter and bladder X-ray showing knotting of the proximal part of the JJ stent (red arrow).
A trial of unknotting by insertion of a 0.38 mm regular guidewire passing through the lumen of the stent under guidance of fluoroscopic guidance failed. The insertion of an 8 Fr semi-rigid ureteroscope, which was the smallest available ureteroscopy, did not reach the knot due to limited space. There were no signs of obstruction from the knotted JJ stent. A decision to postpone the operation for another month was made to remove the right JJ stent with one last trial of retrograde removal. Thirty days later, cautious removal of the right knotted JJ stent was undertaken using gentle traction and the stent was removed without complication (Figure 3). Follow up with the urologic clinic did not show any further complications.
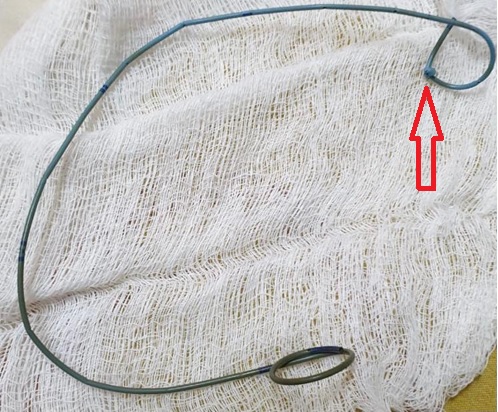
Figure 3: The JJ stent knotted at the proximal part (red arrow) after successful removal by gentle traction.
Discussion:
Complications with stent use is a commonly reported problem in the field of endourology. Common stent complications include dysuria, flank pain, vesicoureteral reflux, urinary tract infection or obstruction, stent migration, stent encrustation and stent fragmentation (5). Meanwhile, ureteral knotting of the JJ stent during retrieval of the stent is a rare and challenging incidence and a careful approach should be carried out accordingly. Trial of the removal of the JJ stent while it is knotted may cause unwanted complications such as avulsion of the ureter or stent cutting. The etiology of JJ stent knotting is unclear. According to the literature, the cause may be due to the length of the stent itself. Other studies have reported that it is often seen with a JJ stent sized 4.7 to 7 Fr, which is a commonly used size in the practice of ureteral stenting (4). Redundant stent is considered as a possible cause of knotting in patients with short ureters after ileal conduit, ureteric reimplantation, and renal transplantation (6). The optimal sized JJ stent would reduce the risk of JJ stent knotting. However, there are still no guidelines that have been implemented in the management of JJ stent knotting. Non-careful management can result in serious complications such as major ureteric injury or loss of the kidney (7). Different techniques have been used to manage this complication, including gentle traction, percutaneous removal, open ureterotomy, using a holmium laser and antegrade removal of a knotted stent (8). In the literature, evidence regarding gentle traction of the knotted stent shows promising results and complete removal without complications (9). However, there is a risk of ureteral trauma when using gentle traction and it should be avoided, especially if the surgeon finds strong resistance (10). In our case, gentle traction was undertaken by an experienced urologist bearing in mind the possibilities of any complications beforehand before it arose, especially if strong resistance was encountered.
Conclusion:
Knotted ureteral stents are a rare complication. A variety of management methods have been sought and are successful, including antegrade removal of a knotted stent, percutaneous removal, open ureterotomy, and using a holmium laser. Gentle traction is considered safe and easy if done with the right operator and enough experience. This choice of management might relieve the patient of other invasive methods. However, it comes with a risk of major ureteric injury such as avulsion or kidney injury and should be planned carefully.
Declaration
Statement:
The authors declare no conflict of interest.
Funding:
None
Ethical Consideration:
An informed written consent was taken from the patient to report this case without revealing any personal information and an ethical approval was obtained from Dammam Medical Complex Institutional Review Board to publish this case.
Data Availability:
All data is available withing the article.
