Volume 3, Issue 11
November 2023
Prevalence of Emotional Abuse Among Medical Students in King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Ali Ibrahim Al-Farhan, Fay Khalid Alowid, Faris A. Alkhudairy, Mouath Ahmed Alturaymi, Ali Zakariya Al-Salam, Khalid Mansour Alduraibi
DOI: http://dx.doi.org/10.52533/JOHS.2023.31111
Keywords: Abuse, emotional, medical students, prevalence, Saudi Arabia
Background: Emotional abuse is often described as a precursor to physical abuse and has a significant negative impact on individuals' well-being. This is a widespread issue, especially in the educational context. The study aims to investigate the prevalence of emotional abuse among medical students at King Saud bin Abdulaziz University of Health Sciences in Riyadh, Saudi Arabia.
Methods: A cross-sectional study was conducted among medical students using a survey designed on Google Forms. The data was analyzed using SPSS software version 27. Medical students in their third and sixth years of education were included in the study, while students unwilling to participate and questionnaires with missing responses or data were excluded from the study. Additionally, students from any research team were also excluded.
Results: A total of 227 medical students participated in the study, comprising 105 men and 122 women. The majority of students (87.2%) knew about emotional abuse. The prevalence of emotional abuse reported in our study population was 6.4%, with only 0.8% suffering from severe abuse. Based on Fisher's exact test results, none of the examined factors—gender, smoking status, substance use, mental health disorders, GPA, and stream—showed significant associations with emotional abuse among medical students in this study (p-value > 0.05)
Conclusions: This study observed a comparatively lower prevalence of emotional abuse in our setting. However, detecting emotional abuse among medical students is essential to protecting their mental health, academic progress, professional development, and the well-being of future patients. It also aligns with the ethical standards and principles of professionalism that are central to the medical profession.
Introduction
Early childhood trauma can generate persistent issues that persist into adulthood by drastically altering a child's normal development. Studies have revealed a link between childhood trauma and symptoms that might last into adulthood on the physical, mental, sexual, and emotional levels. The most difficult and common type of child abuse and neglect, according to the American Academy of Pediatrics, is psychological maltreatment since it is harder to identify. Because of its very nature, emotional abuse can be insidious and go unrecognized. Perhaps the most harmful kind of abuse, emotional abuse, is frequently misinterpreted and can have long-term effects on adults (1). A meta-analysis of a worldwide study reported rates of 12.7% for sexual abuse, 16.3% for physical neglect, 18.4% for emotional neglect, 22.6% for physical abuse, and 36.3% for emotional abuse (1, 2).
Emotional abuse targets the emotional and psychological well-being of the victim, and it is often a precursor to physical abuse. There is a notable relationship between physical and emotional abuse, and abuse early in a relationship predicts that physical abuse may happen later in the relationship (3, 4). Emotional abuse not only causes low self-esteem but also impacts the nervous system. Emotional abuse causes alterations in the brain, particularly in regions associated with understanding, controlling, recognizing, and responding to the emotions of others. Thinning in the tissue of the brain that is associated with self-awareness and emotional regulation, specifically in the prefrontal cortex and medial temporal lobe. Individuals who report a history of emotional abuse often have painful memories of the abuse which lead to negative feelings. It has been reported that people who have suffered from emotional abuse experience depression, anxiety, a sense of worthlessness, moodiness, and inappropriate emotional responses (5, 6).
Victims of emotional abuse isolate themselves due to the repeated threats, manipulation and intimidation that are caused by another person. In addition, victims of emotional abuse may feel anxious and will start blaming themselves as well as feeling unworthy. Emotional abuse can be difficult to detect since there are no physical signs of it (7). It is often a misinterpreted form of trauma. Emotional abuse can be the most damaging type of abuse since it leads to long-term damaging effects for adults (6).
Few studies dealt with the subject of emotional abuse among university students. Kimber et al. (2017) aimed, through their studies, to find out the association of emotional abuse with abuse among university students. The study sample included 777 students. The study found that one in 10 students (10.7%) had experienced emotional abuse in the past year. It also found that emotional abuse was linked to gender, age, and recent marijuana use (7).
Karakurt and Silver (2013) aimed to find out the relationship between sex and age on emotional abuse in intimate relationships. This study included 250 participants. The study found that younger men experienced higher levels of emotional abuse. Older females experienced less emotional abuse than older males (6).
Patterson et al. (2022) aimed to examine the factors related to emotional abuse by an intimate partner among a sample of university students. The research sample included 1357 undergraduate students from two universities in the United States. The study found that white and older female students are more likely to experience emotional abuse. Also, students witnessing their father abuse their spouse, frequent use of pornography, increased alcohol use, and frequent flings increased the odds of emotional abuse (8).
Rich et al. (1997) aimed to find out the impact of long-term childhood emotional abuse among university students. The study included a sample of 90 college students with questionnaires regarding their history of abuse and their current psychological functioning (Revised 90 Symptom Checklist). It was found that childhood emotional abuse, even in the absence of any other type of abuse, was significantly associated with negative long-term outcomes for these students. Survivors of childhood emotional abuse were more depressed than people who did not report childhood abuse. In addition, survivors reported significantly more general psychopathological symptoms than those who did not report experiencing childhood abuse (9).
Li et al. (2021) aimed to explore the mediating effects of emotional and behavioral problems on the association between childhood emotional abuse and depressive symptoms among university students. Data were drawn from 60 universities from 10 provinces in China (total number of participants = 30,374). Based on the Childhood Trauma Questionnaire (CTQ-SF), the Center for Epidemiological Studies Depression Scale (CES-D) and the Strengths and Difficulties Questionnaire (SDQ). The study found that childhood emotional abuse was strongly associated with depressive symptoms in college students. Of the five identified subtypes of emotional and behavioral problems, four subtypes mediated the relationship between child emotional abuse and depressive symptoms, including affective problems, hyperactivity, peer problems, and prosocial behavior (10).
Eskici and Tinkir (2019) aimed to determine the level of exposure to emotional violence among university students. In addition to trying to identify the relationship between the level of exposure to emotional violence and the variables of university students' age and gender, whether they received psychological support before and after university, and the school they attend. Around 701 undergraduate students participated in the survey. The study data was collected using the “Emotional Violence Scale” which was developed within the scope of the research. The study found a low level of exposure of university students to emotional violence. In addition, it was concluded that the exposure of male students to emotional violence was significantly higher than that of female students. It was also concluded that the students who were exposed to emotional violence had statistically significant differences according to the variables (2). Physical and sexual abuse are often highlighted, whereas a strong stigma surrounding emotional abuse remains unaddressed, despite its significant association with individuals' mental health. This study aims to assess the incidence of emotional abuse among medical students in our setting, Saudi Arabia. The findings of this study may contribute to the design and development of counselling programs and support groups that can benefit affected individuals.
Methods
This cross-sectional research study was conducted over a three-month period at King Saud bin Abdulaziz University for Health Sciences (KSAU-HS) in Riyadh from 1st of March 2023 to 3rd of August 2023. Questionnaire responses were collected and analysed. During the study, participants were made aware of the nature and rationale of the research. Confidentiality was assured throughout the study period. Prior to conducting the study, consent forms were presented to participants, and authorization was obtained. The sample size was determined using Richard's equation at a 5% significance level, employing a simple random sampling technique. Data collection was carried out using Google Forms, with anonymized data and systematic sampling methods. Medical students in the third and sixth years of education were included in the study, while students unwilling to participate and questionnaires with missing responses/data were excluded. Additionally, students who were part of any research team were also excluded.
In Saudi Arabia, students have to go through a series of preparatory courses before starting medical school. In our study, students from KSAU-HS were surveyed. The system in that university has medical start their basic science medical education during years 3/4 (equivelant to M1/M2 years in the United States), and transition to their clinical phase years by years 5/6 (equivalent to M3/M4). Our research is aimed to test the difference between students from the start and end of their proper medical education journey.
Study Tool
Neil Jacobson and John Gottman developed a questionnaire on emotional abuse, which was utilized in our study to collect responses. It included 28 items in the survey. A 4-point Likert scale is used to rate each item: Never = 1, Rarely = 2, Occasionally = 3, and Very often = 4. A participant is said to have experienced emotional abuse if her score falls between 73 and 94. A score of more than 95 denotes serious emotional abuse of the subject. This tool has a 0.92 internal consistency and has been validated in previous studies (11).
Statistical analysis
The statistical analysis was performed using SPSS version 26. To evaluate the normality of the data, we employed the Shapiro-Wilks test, which compares the cumulative distribution function of the variable with the theoretical normal distribution. If the p-value exceeds the predetermined significance level, it supports the assumption of normality. Descriptive statistics, including median and interquartile range (IQR), are presented for Age and the total score of Emotional abuse. Frequency and percentages are reported for categorical variables related to demographic characteristics such as gender, smoking, use of any substances, psychiatric disorders, GPA, stream, and questions pertaining to Emotional abuse and its categories. The Fisher exact test was utilized to explore significant associations between the variable of emotional abuse categories and various demographic variables, with accompanying frequencies and percentages. Furthermore, Binary logistic regression was applied to predict the relationship between dependent and predictor variables, providing Odds ratios and 95% confidence intervals. A p-value < 0.05 was considered statistically significant.
Ethical Consideration
The ethical approval from the institutional review board (IRB) was obtained prior to the initiation of the study and was assigned IRB number IRB/0564/23 and study number NRC23R/086/01. An informed consent was obtained from all participants to be included in the study. Those who did not approve were excluded. Furthermore, all answers to the survey were anonymously done with no private data collected or shared. The approval sheet included that participation is voluntary and participants have the right to not complete the survey without giving any reason and this will not affect their current or future status at the university.
Results
|
Table 1: Demographic characteristics of the participants |
|
|
Variables |
Median(Q1, Q3) |
|
Age |
23(22-24) |
|
Variables |
n (%) |
|
Gender |
|
|
Male |
64(51.2) |
|
Female |
61(48.8) |
|
Do you know what is emotional abuse? |
|
|
Yes |
109(87.2) |
|
No |
6(4.8) |
|
Not sure |
10(8.0) |
|
Are you a smoker? |
|
|
Yes |
20(16.0) |
|
No |
105(84.0) |
|
Do you use any of these substances? |
|
|
amphetamines |
3(2.4) |
|
cannabis, Alcohol |
1(0.8) |
|
No, I don't use any of these |
121(96.8) |
|
Social Anxiety disorder |
|
|
No |
112(94.12) |
|
Yes |
7(5.88) |
|
Major depressive disorder |
|
|
No |
105(88.24) |
|
Yes |
14(11.76) |
|
Generalized anxiety disorder |
|
|
No |
107(89.92) |
|
Yes |
12(10.08) |
|
Other psychiatric disorder |
|
|
No |
106(89.08) |
|
Yes |
13 (10.92) |
|
None |
|
|
No |
42(35.29) |
|
Yes |
77(64.71) |
|
GPA |
|
|
less than 4 |
10(8.0) |
|
4-4.24 |
24(19.2) |
|
4.25-4.49 |
26(20.8) |
|
4.5-4.74 |
42(33.6) |
|
above 4.75 |
23(18.4) |
|
Stream |
|
|
1 |
107(85.6) |
|
2 |
18(14.4) |
n: number
Table 1 outlines the demographic details and diverse characteristics of medical students at King Saud bin Abdulaziz University. The participants, with a median age of 23 years (Q1-Q3: 22-24), predominantly exhibit awareness of emotional abuse (87.2%). The gender distribution shows 51.2% male and 48.8% female students, while a substantial majority do not smoke (84.0%). Minimal substance use is reported, with 2.4% using amphetamines, 0.8% using cannabis or alcohol, and 96.8% abstaining. The prevalence of mental health disorders is relatively low, with the majority indicating the absence of social anxiety disorder (94.12%), major depressive disorder (88.24%), generalized anxiety disorder (89.92%), and other psychiatric disorders (89.08%). Notably, 64.71% report no psychiatric disorders. Academic performance varies, with 33.6% falling within the GPA range of 4.5-4.74. The majority of students (85.6%) belong to Streams 1, while 14.4% are in Stream 2 (Table 1).
The stress perceived by medical students, expressed through questions /phrases, is categorized into four frequency levels: never, rarely, occasionally, and very often. A substantial majority (88.8%) of participants believe that emotional abuse is as harmful as physical abuse, and 78.4% acknowledge the potential escalation of emotional abuse to physical abuse. Notably, 12.0% express concern when a close person remains quiet, while 5.6% report feeling emotionally abused when compared unfavourably to others or questioned about the genuineness of their love. Instances of verbal attacks on personality (4.8%), humiliation in front of others during escalated arguments (4.0%), and reckless driving during anger (4.0%) are reported, emphasizing the diverse nature of emotional abuse experiences. Although the majority report never or rarely experiencing these behaviours, it is crucial to recognize that even occasional instances of emotional abuse can significantly impact individuals' emotional well-being and mental health. These findings underscore the importance of seeking appropriate medical assistance and support for individuals facing such experiences and behaviours (Table 2).
|
Table 2: The Frequency distribution of responses to questions of Emotional Abuse |
|
|
Variables |
n(%) |
|
Do you believe that emotional abuse is as harmful as physical abuse? |
|
|
Yes |
111(88.8) |
|
No |
11(8.8) |
|
I don’t know |
3(2.4) |
|
Do you believe that emotional abuse can escalate to physical abuse? |
|
|
Yes |
98(78.4) |
|
No |
1(0.8) |
|
Maybe |
26(20.8) |
|
Those around me/close to me try to catch me at inconsistencies to show that I am lying |
|
|
Never |
57(45.6) |
|
Rarely |
50(40.0) |
|
Occasionally |
16(12.8) |
|
Very often |
2(1.6) |
|
Those around me/close to me try to convince other people that I am crazy |
|
|
Never |
106(84.8) |
|
Rarely |
11(8.8) |
|
Occasionally |
6(4.8) |
|
Very often |
2(1.6) |
|
Those around me/close to me tell other people that there is something wrong with me |
|
|
Never |
82(65.6) |
|
Rarely |
26(20.8) |
|
Occasionally |
15(12.0) |
|
Very often |
2(1.6) |
|
Those around me/close to me say things that hurt me out of spite |
|
|
Never |
57(45.6) |
|
Rarely |
40(32.0) |
|
Occasionally |
24(19.2) |
|
Very often |
4(3.2) |
|
Those around me/close to me insult my ethnic background |
|
|
Never |
96(76.8) |
|
Rarely |
17(13.6) |
|
Occasionally |
8(6.4) |
|
Very often |
4(3.2) |
|
Those around me/close to me insult my family |
|
|
Never |
102(81.6) |
|
Rarely |
17(13.6) |
|
Occasionally |
5(4.0) |
|
Very often |
1(0.8) |
|
Those around me/close to me talk me into doing things that make me feel bad afterwards |
|
|
Never |
76(60.8) |
|
Rarely |
35(28.0) |
|
Occasionally |
11(8.8) |
|
Very often |
3(2.4) |
|
Those around me/close to me tell me no one else would ever want me |
|
|
Never |
98(78.4) |
|
Rarely |
19(15.2) |
|
Occasionally |
6(4.8) |
|
Very often |
2(1.6) |
|
Those around me/close to me humiliate me in front of others |
|
|
Never |
79(63.2) |
|
Rarely |
32(25.6) |
|
Occasionally |
9(7.2) |
|
Very often |
5(4.0) |
|
Those around me/close to me make me do degrading things |
|
|
Never |
103(82.4) |
|
Rarely |
16(12.8) |
|
Occasionally |
5(4.0) |
|
Very often |
1(0.8) |
|
Those around me/close to me question my sanity |
|
|
Never |
96(76.8) |
|
Rarely |
17(13.6) |
|
Occasionally |
8(6.4) |
|
Very often |
4(3.2) |
|
Those around me/close to me tell other people personal information or |
|
|
Never |
72(57.6) |
|
Rarely |
42(33.6) |
|
Occasionally |
10(8.0) |
|
Very often |
1(0.8) |
|
Those around me/close to me verbally attack my personality |
|
|
Never |
59(47.2) |
|
Rarely |
38(30.4) |
|
Occasionally |
22(17.6) |
|
Very often |
6(4.8) |
|
Those around me/close to me have insulted me by telling me that I am incompetent (stupid) |
|
|
Never |
81(64.8) |
|
Rarely |
29(23.2) |
|
Occasionally |
11(8.8) |
|
Very often |
4(3.2) |
|
Those around me/close to me ridicule me |
|
|
Never |
91(72.8) |
|
Rarely |
20(16.0) |
|
Occasionally |
12(9.6) |
|
Very often |
2(1.6) |
|
Those around me/close to me force me to do things against my will |
|
|
Never |
86(68.8) |
|
Rarely |
28(22.4) |
|
Occasionally |
8(6.4) |
|
Very often |
3(2.4) |
|
Those around me/close to me question whether my love is true |
|
|
Never |
83(66.4) |
|
Rarely |
20(16.0) |
|
Occasionally |
15(12.0) |
|
Very often |
7(5.6) |
|
Those around me/close to me compare me unfavourably to other people |
|
|
Never |
73(58.4) |
|
Rarely |
26(20.8) |
|
Occasionally |
19(15.2) |
|
Very often |
7(5.6) |
|
Those around me/close to me intentionally do things to scare me |
|
|
Never |
99(79.2) |
|
Rarely |
16(12.8) |
|
Occasionally |
9(7.2) |
|
Very often |
1(0.8) |
|
Those around me/close to me threaten me physically during arguments |
|
|
Never |
100(80.0) |
|
Rarely |
16(12.8) |
|
Occasionally |
7(5.6) |
|
Very often |
2(1.6) |
|
Those around me/close to me warn me that if I keep doing something, violence will follow |
|
|
Never |
102(81.6) |
|
Rarely |
11(8.8) |
|
Occasionally |
10(8.0) |
|
Very often |
2(1.6) |
|
My arguments often escalate out of control |
|
|
Never |
72(57.6) |
|
Rarely |
38(30.4) |
|
Occasionally |
10(8.0) |
|
Very often |
5(4.0) |
|
I’m worried most when a close person is quiet |
|
|
Never |
56(44.8) |
|
Rarely |
26(20.8) |
|
Occasionally |
28(22.4) |
|
Very often |
15(12.0) |
|
Those around me/close to me drive recklessly or too fast when they are angry |
|
|
Never |
64(51.2) |
|
Rarely |
35(28.0) |
|
Occasionally |
21(16.8) |
|
Very often |
5(4.0) |
n: numbers
Table 3 illustrates the distribution of students' exposure to emotional abuse, revealing a prevalence of 5.6% reporting emotional abuse and an additional 0.8% classified as 'Severely abused.' Thus, the total prevalence of emotional abuse reported in our study population was 6.4%, with only 0.8% suffering from severe abuse. These findings emphasize that a small, yet noteworthy proportion of students have encountered emotional abuse. The total emotional abuse scores, with a median of 34 (range: 27-44.50), underscore the diverse range of experiences among medical students, providing valuable insights into the nuanced nature of emotional abuse within the study population (Table 3).
|
Table 3: Frequency distribution of Students' Exposure to Emotional Abuse |
|
|
Emotional abuse |
n(%) |
|
Not emotionally abused |
117(93.6) |
|
Emotionally abused |
7(5.6) |
|
Severely abused |
1(0.8) |
|
Emotional Abuse total score Median(Q1-Q3) |
34(27- 44.50) |
Figure 1 illustrates the percentage of students exposed to emotional abuse, categorized based on their scores. According to our statistical calculations, the results demonstrate that 93% of participants did not experience emotional abuse, as their total scores were below 73. Around 6.4% of students indicated experiencing emotional abuse, with 5.6% specifically reporting emotional abuse and an additional 0.8% categorized as having experienced severe abuse. These scores were within the range of 73 to 95 (Figure 1).
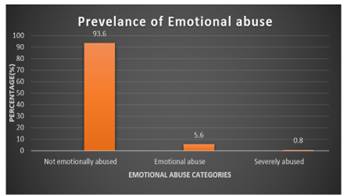
Figure 1: The percentage of students’ exposure to emotional abuse
Fisher's exact test was applied to examine the significant relationship between emotional abuse categories and other demographic variables. Among the participants studied, males (28.57%) were emotionally abused, females (71.43%) were emotionally abused, and none were severely abused. The p-value is 0.266 > 0.05. Therefore, gender is not significantly associated with emotional abuse. There was no significant association between smoking status and emotional abuse. Both among those who smoke and those who do not smoke, the proportions of those who experienced emotional abuse are similar. The p-value is 1.000, indicating a lack of significant association. Similarly, there is no significant association between substance use (amphetamines or cannabis/alcohol) and emotional abuse. Regardless of substance use, the proportions of emotional abuse are similar. The p-value is 1.000, indicating no significant association. For Mental Health Disorders (Social Anxiety disorder, Major depressive disorder, Generalized Anxiety disorder, other psychiatric disorders): None of these mental health disorders appear to be significantly associated with emotional abuse. The p-values are all greater than 0.05, indicating a lack of significant association. Whether individuals have none of the listed psychiatric disorders or not does not show a significant association with emotional abuse. The p-value is 0.095 > 0.05, indicating no significant association. GPA categories do not exhibit a significant association with emotional abuse. The p-value is 0.543, indicating no significant association. Stream also does not show a significant association with emotional abuse with a p-value of 1.000, indicating no significant association. Hence based on Fisher's exact test results, none of the examined factors (gender, smoking status, substance use, mental health disorders, GPA, and stream) are significantly associated with emotional abuse among medical students in this study. This suggests that these factors may not be strong predictors of emotional abuse within this specific population or that the sample size may not be sufficient to detect significant associations if they exist (Table 4).
|
Table 4: Association between emotional abuse and demographic variable among medical students-Fishers exact test |
||||
|
Variables |
Emotional abuse |
|||
|
Not emotionally abused n(%) |
Emotionally abused n(%) |
Severely abused n(%) |
p-value |
|
|
Gender |
||||
|
Male |
61(52.14) |
2(28.57) |
1(100) |
0.266 |
|
Female |
56(47.86) |
5(71.43) |
0(0) |
|
|
Are you a smoker? |
||||
|
Yes |
19(16.24) |
1(14.29) |
0(0) |
1.000 |
|
No |
98(83.76) |
6 (85.71) |
1(100) |
|
|
Do you use any of these substances? |
||||
|
amphetamines |
3(2.56) |
0(0.00) |
0(0) |
1.000 |
|
cannabis, Alcohol |
1(0.85) |
0(0.00) |
0(0) |
|
|
No, I don't use any of these |
113(96.58) |
7(100.00) |
1(100) |
|
|
Social Anxiety disorder |
||||
|
No |
106(95.50) |
5(71.43) |
1(100) |
0.111 |
|
Yes |
5(4.50) |
2(28.57) |
0(0) |
|
|
Major depressive disorder |
||||
|
No |
98(88.29) |
6(85.71) |
1(100) |
1.000 |
|
Yes |
13(11.71) |
1(14.29) |
0(0) |
|
|
Generalized Anxiety disorder |
||||
|
No |
101(90.99) |
5(71.43) |
1(100) |
0.235 |
|
Yes |
10 (9.01) |
2(28.57) |
0 (0) |
|
|
Other psychiatric disorders |
||||
|
No |
100(90.9) |
5(71.43) |
1(100) |
0.262 |
|
Yes |
11(9.91) |
2(28.57) |
0(00) |
|
|
None |
||||
|
No |
37(33.33) |
5(71.43) |
0(0 |
0.095 |
|
Yes |
74(66.67) |
2(28.57) |
1(100) |
|
|
GPA |
||||
|
less than 4 |
9(7.69) |
1(14.29) |
0(0) |
0.543 |
|
4-4.24 |
24(20.51) |
0(0.00) |
0(0) |
|
|
4.25-4.49 |
24(20.51) |
2(28.57) |
0(0) |
|
|
4.5-4.74 |
39(33.33) |
3(42.86) |
0(0) |
|
|
above 4.75 |
21(17.95) |
1 (14.29) |
1(100) |
|
|
Stream |
||||
|
1 |
100(0.85) |
6(85.71) |
1(100) |
1.000 |
|
2 |
17(1.71) |
1 (14.29) |
(0) |
|
A binary logistic regression model was carried out to assess the significant relationship between the outcome and predictor variables i.e., between the emotional abuse variable and demographic factors of medical students. There was no significant relationship between Age, gender, smoking, use of any substance, different psychiatric disorders, GPA, and Emotional abuse as p-value >0.05 (Table 5).
|
Table 5: Logistic regression analysis of factors associated with Emotional abuse |
||
|
Predictor Variables |
Odds Ratio (95% CI) |
p-value |
|
Age |
||
|
Gender (Reference Male) |
1.113(0.161-7.699) |
0.914 |
|
Smoking |
0.894(0.064-12.497) |
0.933 |
|
Use of any substance |
0.000(0.000-0.000) |
1.000 |
|
Social anxiety disorder |
0.130(0.011-1.537) |
0.105 |
|
Major depressive disorder |
5.283(0.189-147.753) |
0.327 |
|
Generalized anxiety disorder |
0.365(0.025-5.363) |
0.462 |
|
Other psychiatric disorder |
0.187(0.015-23.439) |
0.954 |
|
None |
1.499(0.160-14.008) |
1.499 |
|
GPA (Reference less than 4) |
0.583(0.066-5.175) |
0.628 |
OR: Odds ratio; CI: Confidence Interval.
Discussion
This study assessed the incidence of emotional abuse experienced by medical students, further analyzing the trends in psychiatric disorders, substance use, smoking habits, and their education grade point averages. Responses to the emotional abuse questions were scored, and the cumulative score was calculated at the end to determine the severity of the emotional abuse experience. Furthermore, the correlation between emotional abuse and other variables was examined. The results of our study show that the majority of students (87.2%) were knowledgeable about emotional abuse. The incidence of emotional abuse reported in our study population was 5.6%, with only 0.8% experiencing severe abuse.
Findings of another observational study from Saudi Arabia conducted among 241 medical students and 11 interns in 2021 reported that overall, there were 56.9% of violent incidents. Emotional abuse accounted for the majority of violence incidents (50.2%), while emotional and physical abuse together accounted for the largest percentage of abuse cases (14.7%) (12). Results of another study from Saudi Arabia among health sciences university students in 2023 revealed that 42% of individuals were victims of abuse of any kind. The most common type of abuse (51.1%) was physical, which was followed by emotional abuse (49.9%), sexual abuse (29.6%), and a lack of safety and protection (38%) (13). While comparing our results with these two national studies similarly conducted among medical/health sciences students, our reported prevalence of emotional abuse is much lower, which may be due to the differences in sample size. Results of a Saudi Arabian study conducted among young adults in 2022 showed that of the 611 respondents, 24.5% of the males and 48.1% of the females reported experiencing emotional abuse (14).
Furthermore, comparing our findings with the other studies in the literature and drawing comparisons of our results with international studies, the findings of a study from Kuwait in 2020 among 2508 respondents showed that almost 53.5% suffered from emotional abuse (15). Results of a study in Iceland demonstrated that out of the eight various types of emotional abuse, more than two-thirds of adults report having experienced one or more of them (16). Findings of a national survey from Swaziland showed that 28.5% of girls reported experiencing emotional abuse at least once in their lifetime, while 58.3% of them reported experiencing abuse frequently (17). At the same time, findings from a study from Sweden showed that the lifetime prevalence of emotional abuse was 12.8% (18).
Our results, still with the international studies comparison, demonstrated much lower percentages for emotional abuse, which may be due to the limited sample size of the population or underreporting by individuals. Owaidah et al. stated that healthcare professionals and students studying healthcare specializations disclosed that they did not report suspected child maltreatment because they were unsure if abuse had occurred, did not know enough about the issue, thought that injuries were not serious enough to report, were unaware of protocol, had a bad experience after reporting, or did not believe there would be strict legal repercussions for not reporting. It has been observed that abused children seldom report maltreatment to the authorities for a number of reasons, including low self-esteem, a fear of their family disintegrating, or ignorance of the maltreatment's existence in the first place (19). However, in our study majority (87.2%) of the participants were aware of the concept of emotional abuse.
Emotional abuse is a form of child maltreatment that, later in life, increases the risk of mental, cognitive, and behavioral disorders. Since emotional abuse does not involve a specific life incident, such as an injury or accident, it is particularly challenging to document this form of maltreatment. Over time, the consequences of emotional abuse become quite apparent, involving impaired emotional, social, and cognitive development. This maltreatment category often overlaps with physical injury (20). Studies have indicated that those who are subjected to emotional abuse have an increased likelihood of developing depressive symptoms as adults (21). Findings from another study also demonstrated that depression was found to be directly correlated with emotional abuse, and social anxiety played a role in mediating this relationship (22).
In this study, however, we did not find any significant association between emotional abuse and mental disorders, although almost 11.76% of participants had major depressive disorder, 10.08% had generalized anxiety disorder, 10.92% had other psychiatric disorders, and 5.88% suffered from social anxiety disorder, despite the low prevalence of emotional abuse observed in our study. This may be due to the fact that since medical schools are typically demanding for students, it has been assumed that medical students suffer from depression at higher rates than other students. Almost one-third of medical students worldwide suffer from depression, yet few receive treatment for it (23).
Results of another cross-sectional study from Saudi Arabia among 2562 respondents in 2018 demonstrated that, compared to individuals in other specializations, medical students reported a depression rate that was 25% greater. While the prevalence of stress among Saudi medical students was 57% (24), Mirza et al., while reviewing the literature, reported that a recent meta-analysis estimated that 27.2% of medical students worldwide experienced depression or one of its forms. According to the results of another systematic analysis, the prevalence of depression ranged from 6.0% to 66.5%. A study conducted in the United Arab Emirates investigated anxiety and depression in medical professionals, students, and staff at the Medical College for Girls. They observed that 7.8% of medical staff members and 28.6% of medical undergraduates had significant depression scores. Hence, the overall prevalence of depression or its symptoms among medical undergraduates varied from 1.4% to 73.5% overall (25). Moutinho et al., in their cross-sectional study among 761 respondents, also reported that medical students exhibit high levels of stress, anxiety, and depression symptoms, with notable variations between semesters (26). The prevalence of depression and other psychiatric disorders observed in our study sample population is lower than reported in the literature.
In terms of substance abuse, only a minority of medical students were involved, as only 2.4% took amphetamines and only 0.8% consumed alcohol and cannabis. On the contrary, results of another cross-sectional study among medical students from Lebanon reported that substance abuse was present in 20.43% (27). Similarly, results of another cross-sectional Iranian study among 1149 university students demonstrated that the most often used substances among the students were alcohol (14.0%), tobacco (28.3%), and cannabis and marijuana (5.2%) (28). Findings of a study from India also revealed a higher percentage (20.73%) of substance abuse among medical students (29).
Roncero et al., while describing findings from literature on substance abuse among medical students, stated that the three most commonly used substances are cannabis (11.8%), tobacco (17.2%), and alcohol (24%). Additionally common (9.9%) is the usage of hypnotic and sedative medications. Stimulant use is 7.7%, cocaine use is 2.1%, and opiate use is quite low at 0.4%. Up to 14.1% of individuals use inhalants in some regions of Latin America. The rate of substance use among students in their last years of education is greater. With the exception of hypnotics and sedatives, men are more likely than women to use drugs. Therefore, medical students’ substance abuse is a phenomenon that has to be thoroughly investigated because of its frequency and possible consequences (30). Moreover, our study did not report any significant association between substance use and emotional abuse.
It is well known that abuse and mistreatment of medical students is a serious issue in medical schools (31). Henry Silver first commented on the mistreatment of medical students in 1982, drawing attention to how similar it was to child abuse. According to later research, the majority of American medical students encounter mistreatment of some kind while undergoing training. Mistreatment reports include physical intimidation, public humiliation, and discrimination based on race and gender (32). This mistreatment can also be a contributing factor to emotional abuse and the incidence of psychiatric disorders among medical students; however, special attention to emotional abuse among medical students necessitates further research as studies in the literature are quite limited in this regard. Medical education should foster a positive and supportive learning environment that encourages collaboration, empathy, and personal growth. Detecting and addressing emotional abuse contributes to creating a more respectful and inclusive educational atmosphere that benefits all students. Our study highlights the important concept of emotional abuse among medical students, which has historically received limited attention. This research can assist institutions in early identification and detection of emotional abuse and psychiatric disorders among individuals by regularly conducting such surveys among students. However, our study has certain limitations. Firstly, the findings are based on self-reported measures, which can introduce bias through over-reporting or under-reporting. Secondly, being a single-center study with a limited sample size limits the generalizability of our findings to other settings and necessitates further research with larger study samples at multi-center levels.
Conclusion
This study observed a comparatively lower prevalence of emotional abuse in our setting. However, detecting emotional abuse among medical students is essential to protect their mental health, academic progress, professional development, and the well-being of future patients. It also aligns with the ethical standards and principles of professionalism that are central to the medical profession. Further research is needed to delve deeper into the underlying factors contributing to emotional abuse and develop targeted interventions to effectively address this issue among medical students.
Disclosure
Conflict of Interest
The authors declare no conflict of interest.
Funding
No funding
Author Contribution
All authors contributed equally to conceptualizing, study design, data collection, data coding, data analysis, writing and proofreading of the manuscript.
Ethical Consideration
The ethical approval from the institutional review board (IRB) was obtained prior to the initiation of the study and was assigned IRB number IRB/0564/23 and study number NRC23R/086/01. An informed consent was obtained from all participants to be included in the study. Those who did not approve were excluded. Furthermore, all answers to the survey were anonymously done with no private data collected or shared. The approval sheet included that participation is voluntary and participants have the right to not complete the survey without giving any reason and this will not affect their current or future status at the university.
