Volume 2, Issue 11
November 2022
Fracture Patterns in Saudi Arabian Road Traffic Accidents Over the Last 12 Years: A Systematic Review
Hamed Al Nefaie, Zuhair Alsuhaymi, Ahmed Alzahrani, Abdulaziz Alghamdi, Emtenan Esmael, Nuran Eid, Eyad Agheel, Fatimah ALJuraysan, Naif Alrawaili, Nuha Alasmari, Atheer Alasmary, Noha Attiah
DOI: http://dx.doi.org/10.52533/JOHS.2022.21113
Keywords: road traffic accidents, fracture, Saudi Arabia, pattern
Background: Road traffic accidents are a major non-communicable epidemic that accounts for death and morbidity in the world today. Despite considerable attention given to health statistics of road traffic accidents (RTAs), the pattern of bone fracture aspects of injuries resulting from RTAs is not fully understood in Saudi Arabia. This review aimed to study the epidemiological pattern of fractures due to RTAs in Saudi Arabia.
Methods: This systematic review was based on the latest evidence of RTA fractures in the Kingdom of Saudi Arabia (SAUDI ARABIA). All articles published during the last 12 years on road traffic accident-associated fractures in SAUDI ARABIA were analyzed. We examined 12 studies published between 2012 and 2022. Eleven included studies were cross-sectional studies and collected data retrospectively, while one study was a cohort.
Results: A total of 4709 patients with fractures admitted in 2010–2022, followed by road traffic accidents, were included. Male patients accounted for 81.6% (n = 3843) of all fractures reported. The most commonly fractured body areas were the upper limb extremities (30.05%), followed by lower limb extremities (11.30%), head or skull fracture (10.53%), spine fracture (8.83%), ribs fracture (8.52%), neck fracture (8.09%), pelvis fracture (3.44%), clavicle fracture (1.89%), and sternal fracture (0.28%). Among the upper limb fractures, the femur bone was most fractured (17.06%), and the combined tibia patella and fibula accounted for 17.69% of upper limb fractures.
Conclusion: Lower limb fractures, especially femur bone fractures, are prevalent in Saudi Arabia, and caused by RTAs, especially among young males. Therefore, the concerned authorities need to employ and implement stricter traffic rules to minimize the risk of RTA fractures and their subsequent increased morbidity and mortality rates.
Introduction
According to the Global Status Report on Road Safety 2018, Saudi Arabia had the highest death rate associated with road injuries of any high-income country in 2016, at an estimated 28.8 per 100,000 population, with a total count of fatalities of 9,031. Despite precautionary efforts and programs, RTA is a leading major cause of morbidity and mortality in Saudi Arabia (1). Road traffic accidents contribute to 81% of the deaths of hospitalized patients in SAUDI ARABIA. In Saudi Arabia, RTAs result in about four injuries every hour and more than 19 fatalities each day (2).
Motor vehicle accidents (MVAs) are the main cause of trauma in Saudi Arabia and worldwide. According to WHO, there are numerous global risk factors for RTAs, including speeding, operating a vehicle while under the influence of psychoactive substances, not using a seatbelt, child restraints, or being distracted by a phone while driving, unsafe vehicles and road infrastructure, inadequate post-crash care, and insufficient traffic law enforcement (3). Around four people are injured per hour, and 81% of total hospital fatalities are due to MVAs (4), with most victims being young adults, causing devastating social, economic, and health consequences. The most frequent injuries among patients admitted as a result of road RTAs were orthopedic fractures. In comparison to non-MVA cases, MVA cases had considerably higher rates of ICU admissions, higher rates of additional injuries, and lower Glasgow Coma Scale (GCS) values. These findings demonstrate that MVAs are a significant public health issue with serious effects on hospital resources and people's quality of life (5, 6).
Some of the causes of unsafe driving practices and traffic violations are prevalent cultural and lifestyle elements. By 2030, it is anticipated to rank as the fifth most common cause of death (7, 8). Recent statistics show that nationwide, road accidents result in greater than 19 fatalities each day and about 4 injuries every hour. Human factors, including speeding, breaking traffic laws, and being fatigued, are the main causes of the rise in death rates (9, 10). Additionally, as the population develops, there are more motor vehicles on the road (11). Major orthopedic injuries (OIs) are linked to faster speeds and more frequent hospital admissions. Currently, the head/skull and neck, followed by the upper and lower limb areas, are the body parts most often affected (1).
The goal of the current study was to describe the orthopedic fracture pattern among RTA victims including both adults and children in the Saudi Arabian region.
Methods
Definition of outcomes and inclusion criteria
Either retrospective or prospective cross-sectional and cohort studies on the pattern of traffic fractures, as well as research done in Saudi Arabia and English-language literature, were required for inclusion in the study. The exclusion criteria for this study were conference presentations, case reports, interventional studies, economic studies, clinical studies, management studies, and other studies without an epidemiological pattern. Articles that collected data earlier than the year 2010 were not included due to the possibility of transitions in epidemiological patterns.
Search strategy
Multiple databases, including PubMed/Medline, Google Scholar, and the Cochrane Library, were searched for pertinent literature. For the search, the following precise keywords were used, either separately or in combination: “traffic accidents” OR “traffic crashes” OR “motorcycle accident” OR “motorcycle crash” OR “motorcycle injury” OR “trauma” OR “fracture” OR “injury” OR “injuries” AND “Saudi Arabia” OR “Kingdom of Saudi Arabia” OR “KSA” OR “Saudi”. To make the search more precise, Boolean operators were also used. In order to use just the pertinent research, our search method was restricted to the title and abstract of the search results. All of these findings were saved to an Endnote library so that we could find and use any duplicate entries across the many databases we searched. In addition, we manually searched every similar article section in PubMed, including studies and pertinent reviews, in the hopes of finding any research that the primary electronic search approach could have overlooked. This systematic review's stages were all carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (12).
Screening and extraction
Articles with no relevant titles were excluded. In the second phase, the abstract and full text of articles were reviewed to include those articles matching the inclusion criteria. Reference management (Endnote X8) was used for organizing and assessing the titles and abstracts, as well as for identifying any duplicate entries. To preserve excellent quality in this crucial phase, we adopted a double screening technique, one for evaluating titles and abstracts and the other for assessing whole texts. An orderly extraction sheet that was pertinent to our desired outcomes was created after making sure that all pertinent articles were included. The sheet contained the baseline traits and the desired results. The baseline characteristics consisted of study design, sample size, source of data, study conducted region, gender, and age distribution. The determined outcomes of this study included fractures of various body sites: head or skull; neck; maxillofacial; upper limb, lower limb; clavicle; spine; ribs; and sternal and pelvis body sites.
Quality assessment
We used the modified Newcastle-Ottawa scale (NOS) for cross-sectional studies and cohort studies (12), which mainly consists of three major domains: including the quality of methods; compatibility; assessment; and reporting of the outcomes. This scale gives each category a maximum of five, two, and three stars, respectively. The selection was assessed based on power estimates, sequential participant selection, and recruiting bias. Comparability was established using studies that included adjustments for either of the following variables: participant age (<40), or gender. It is widely accepted that a maximum of five stars could be used to distinguish studies with little risk of bias. Studies were rated as unsatisfactory studies (0–4), satisfactory studies (5 - 6), good (7 - 8), and very good studies (9 -10), on a scale of 0 to 10, depending on how biased they were.
Search results
We were able to uncover a total of 128 citations using the aforementioned search techniques, which were subsequently reduced to 49 after duplicates were eliminated. Only 24 citations remained after the title and abstract screening that qualified for the following stages. Only 12 publications were found to satisfy our inclusion and exclusion criteria after the full-text screening. Figure 1 displays the thorough search and screening procedure.
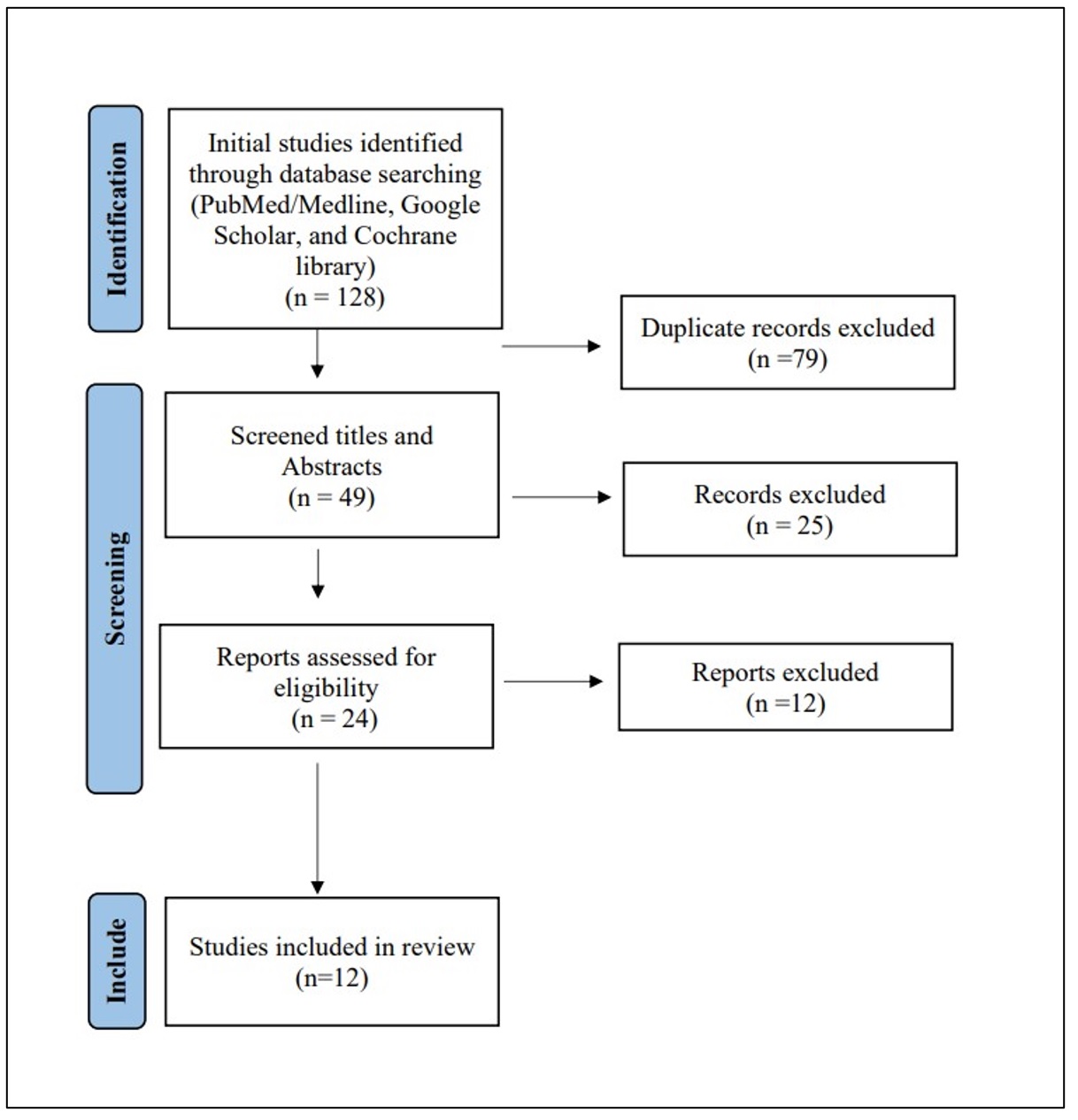
Figure 1: PRISMA flow chart of the included studies
Results of quality assessment
Our assessment of bias for the included studies showed that all the studies scored above five and all of the reviewed studies had good quality (n = 12), which was associated with a lower risk of bias. None of the included studies showed low quality (Table 1).
|
Table 1. Summary of the results of bias assessment of the included studies using the modified Newcastle-Ottawa scale (NOS) for non-randomized observational studies. |
|||||
|
Study |
Selection |
Comparability |
Outcome |
Total Score |
Study Quality |
|
Alotaibi et al. |
**** |
* |
*** |
8 |
good |
|
AbdelRazik et al. |
**** |
* |
*** |
8 |
good |
|
Elnibras et al. |
**** |
* |
*** |
8 |
good |
|
Aloudah et al. |
**** |
* |
*** |
8 |
good |
|
Alraddadi et al. |
**** |
* |
*** |
8 |
good |
|
Algahtany et al. |
**** |
* |
*** |
8 |
good |
|
Alkhthlan et al. |
**** |
* |
*** |
8 |
good |
|
AlHammad et al. |
**** |
* |
*** |
8 |
good |
|
Sonbol et al. |
**** |
* |
*** |
8 |
good |
|
Mohmmedthani et al. |
**** |
* |
*** |
8 |
good |
|
Almansouf et al. |
**** |
* |
*** |
8 |
good |
|
Alghthani et al. |
**** |
* |
*** |
8 |
good |
Characteristics of the study included
We examined 12 studies (6, 9, 13-22) that collected medical record data on fractures due to road traffic accidents between 2010 and 2022 and enrolled 4079 patients. Male patients accounted for 81.6% of all fractures reported. The study regions were Aseer, Riyadh, Al Kharj, Tabuk, Buraydah, and Almadinah in Saudi Arabia. Eleven included studies were cross-sectional studies and collected data retrospectively, while only one included study was a cohort design (Table 2).
|
Table 2. Baseline characteristics of the included studies in this review. |
|||||||
|
STUDY |
Data collection period |
City |
Study design |
Source of data |
Number of included cases |
Age |
Gender |
|
Alotaibi et al. |
2011 - 2016 |
Aseer |
Cross-sectional |
Medical records |
531 |
b29 ± 2 |
485/46 |
|
AbdelRazik et al. |
2018 -2019 |
Al -Kharj |
Cross-sectional |
Medical records |
300 |
< 40 = 246, >40 = 54 |
273/27 |
|
Elnibras et al. |
2010 - 2015 |
Tabuk |
Cross-sectional |
Medical records |
378 |
<40 = 72.5%, > 40 = 27.5% |
323/55 |
|
Aloudah et al. |
2018 - 2019 |
Buraydah |
Cross-sectional |
Medical records |
301 |
<40 = 180, >40 = 143 |
248/53 |
|
Alraddadi et al. |
2011 - 2015 |
Riyadh |
Cross-sectional |
Medical records |
1396 |
a26 (20 -37) |
1200/196 |
|
Algahtany et al. |
2010 - 2020 |
Aseer |
Cross-sectional |
Medical records |
127 |
<45 =104, >45 = 13 |
117/10 |
|
Alkhthlan et al. |
2016 - 2017 |
Al -Kharj |
Cross-sectional |
Medical records |
120 |
<40 = 100, >40 = 20 |
105/15 |
|
AlHammad et al. |
2016 - 2017 |
Riyadh |
Cross-sectional |
Medical records |
372 |
15 - 34 (77%) |
325/47 |
|
Sonbol et al. |
2010 - 2016 |
Almadinah Almunawwarah |
Cross-sectional |
Medical records |
591 |
b33.2 ± 15.9 |
461/130 |
|
Mohmmedthani et al. |
2011 - 2016 |
Almadinah Almunawwarah |
Cross-sectional |
Medical records |
206 |
b6.9 ± 4.1 |
154/52 |
|
Almansouf et al. |
2016 - 2021 |
Riyadh |
Cohort |
Medical records |
203 |
<40 = 105, >40 = 98 |
147/56 |
|
Alghthani et al. |
2010 - 2019 |
Aseer |
Cross-sectional |
Medical records |
184 |
<40 =145, >40=39 |
159/25 |
a: Median; b: Mean
A total of 4709 patients with fractures admitted in 2010–2022, followed by road traffic accidents, were included. The most frequently fractured body sites were the upper limb extremities (30.05%), followed by lower limb extremities (11.30%), head or skull fracture (10.53%), spine fracture (8.83%), ribs fracture (8.52%), neck fracture (8.09%), pelvis fracture (3.44%), clavicle fracture (1.89%), and sternal fracture (0.28%) (Table 3). Among the upper limb fractures, the femur bone was most fractured (17.06%), and the combined tibia patella and fibula accounted for 17.69% of upper limb fractures (Table 4).
|
Table 3. Summary of the fracture sites of the included studies in this review. |
|||||||||||
|
STUDY |
Head/ skull |
Maxillofacial |
Neck |
clavicle |
Upper limb |
Lower limb |
Spine fracture |
Ribs |
Sternal |
Pelvis |
Multiple fractures |
|
Alotaibi et al. |
17 (3.20%) |
NR |
17 (3.20%) |
NR |
170 (32.01%) |
274 (51.60%) |
53 (10%) |
43 (8.1%) |
NR |
58 (10.9%) |
NR |
|
AbdelRazik et al. |
72 (24%) |
NR |
22 (7.33%) |
NR |
NR |
NR |
32 (10.67%) |
70 (23.33%) |
NR |
31 (10.33%) |
35.40% |
|
Elnibras et al. |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
244 (64.6%) |
13 (3.4%) |
NR |
NR |
|
Aloudah et al. |
17 (13.3%) |
NR |
NR |
11 (8.6%) |
NR |
72 (56.2%) |
21 (16.4%) |
14 (10.9%) |
NR |
7(5.5%) |
NR |
|
Alraddadi et al. |
376 (27%) |
NR |
342 (24.5%) |
NR |
299 (21.1%) |
499 (35%) |
190 (14%) |
NR |
NR |
NR |
NR |
|
Algahtany et al. |
14 (11%) |
NR |
NR |
16 (12.6%) |
22 (17.3%) |
40 (31.5%) |
NR |
NR |
NR |
19 (15%) |
23.6% |
|
Alkhthlan et al. |
NR |
NR |
NR |
40 (33.30%) |
14 (11.10%) |
NR |
120 (100%) |
30 (25.13%) |
NR |
NR |
NR |
|
AlHammad et al. |
NR |
mid face= 64%, mandible = 17% |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
|
Sonbol et al. |
NR |
NR |
NR |
NR |
NR |
197 (33.33%) |
NR |
NR |
NR |
NR |
NR |
|
Mohmmedthani et al. |
NR |
NR |
NR |
NR |
NR |
28 (13.59%) |
NR |
NR |
NR |
NR |
NR |
|
Almansouf et al. |
NR |
NR |
NR |
NR |
NR |
267 (100%) |
NR |
NR |
NR |
NR |
73.4% |
|
Alghthani et al. |
NR |
NR |
NR |
22 (12%) |
27 (14.7%) |
38 (20.7%) |
NR |
NR |
NR |
47 (25.5%) |
27.2% |
NR: not reported
|
Table 4: Summary of the upper limb fractures reported in studies |
||||||||
|
Pubis |
Acetabulum |
Femur |
Patella |
Tibia |
Fibula |
Foot and phalanx |
metatarsals |
|
|
Alraddadi et al. |
242 (17%) |
257 (18%) (Tibia + Patella + Fibula) |
82 (6%) |
|||||
|
Sonbol et al |
30 (5.08%) |
74 (12.52%) |
24 (4.06%) |
69 (11.68%) |
||||
|
Mohmmedthani et al. |
19 (9.22%) |
1 (0.49%) |
8 (3.88%) |
|||||
|
Almnsouf et al. |
17 (6.4%) |
5 (1.8%) |
84 (31.5%) |
1 (0.4%) |
80 (29.9%) |
37 (13.9%) |
8 (2.9%) |
16 (5.9%) |
|
Aloudah et al. |
41 (32%) |
16 (12.5%) |
15 (11.7%) |
3 (2.3%) |
||||
Discussion
The rise in the number of road transport accidents is a major factor in the rising mortality and morbidity from road transport accidents in Saudi Arabia. The main cause contributing to the rise in the occurrence of mortality and morbidity is due to psychological factors, including speeding, disobeying traffic laws, and weariness. The incidence of fracture is extremely high in road traffic accidents. They are different from those in other traumas. They are closely related to the injury mechanism. It is crucial to understand all aspects, mainly the leading cause, and determine the patterns accordingly. This study's target is to measure and visualize the pattern of orthopedic injuries brought on by RTAs. Shreds of evidence collected from different studies conducted in various cities in Saudi Arabia revealed that lower limb extremities are the most fractured site in RTAs followed by upper limb extremities and head or skull fracture. The distribution of neck fractures, rib fractures, and spine fractures was almost the same. Among the lower limb extremities, the femur was the most fractured orthopedic site.
The severity of this issue can be justified by looking at the data on traffic accidents and fatalities in Saudi Arabia's regions from 2012 to 2022. In Saudi Arabia, the accident-to-injury ratio is 8:6, which is higher than the international standard of 8:1 (4). It was determined that road injuries were the country's most significant concern. The cities with the highest rates of RTA incidents were Riyadh, Jeddah, Makkah, Madinah, and Qassim (1). Therefore, according to the morbidity and mortality records in Ministry of Health (MOH) hospitals, RTA victims occupy 20% of beds, and RTIs are responsible for 81% of hospital deaths (4).
Age and gender distribution
Owing to our systematic review research, the majority of the victims were under 40 years old and were young. In general, males are more likely than females to get RTA. In Elnibras (14), associated injuries including rib fracture and sternal fracture were more commonly affected in males than in females (57.1% vs. 7.75%, p=0.04). Young-aged drivers are more affected by SAUDI ARABIA's utilizing cars for amusement rather than for purposes (1). Studies from other countries have reported comparable age groups. As per the Aloudah et al. (15) study 82.4%, of the males were met with RTAs, and Alotaibi et al. (9) study reported that, i.e., approximately 91%. This is also emphasized by Sonbol et al. (23) where the number reported was 78%. Fractures from car accidents reported by Alraddadi et al. (16) also found that 86% of the fractured patients were male. AlHammad et al. (6) noted that the 15–34 age group, represented 77% of the sample. Gender inequalities in our country are self-explanatory for local driving laws. In certain studies, men used motor vehicles as their main mode of transportation and leisure, whereas women were not permitted to drive at the time the data was collected in some of the included studies. Male victims are more susceptible to RTAs than female ones because males make up most of the drivers in Saudi Arabia. However, compared to women, men experienced the highest incidence of accidents, injuries, and fractures in another global research. A prospective hospital-based study was conducted (Ethiopia) to evaluate the results and injury characteristics of road traffic accident victims at the adult emergency department at Tikur Anbessa specialized hospital, Addis Ababa. The average age of the study participants was 32.15 ± 14.38 years, with a male-to-female ratio of 2.6:1 (24).
Most involved fracture site
The fracture patterns of the Saudi Arabian studies on RTAs that are included reveal considerable overlaps with other RTA-related studies of a similar nature. Gender, age, and the total number of fractures are the major parallels with the pattern of fractures, based on the studies of Aloudah et al. (15) and Sonbol et al.(19). An earlier study conducted in Saudi Arabia found that fractures of the radius and ulna are the most common types of unintentional fractures and dislocations, trailed by fractures of the hand, foot, tibia, fibula, humerus, clavicle, femur, ankle, spine, and pelvis (25). In the current systematic review, it was observed that the most frequently observed bone fracture was in the upper limb, majorly the femur bone followed by the tibia. This is quite consistent with a study conducted in Nigeria. A study of RTAs and fractures in Nigeria found that the most fractured bone is the femur, followed by the tibiofibular, humerus, tibia, and then the clavicle (26).
Algahtany et al. (17) reportedly found that orthopedic fractures more frequently occurred in the lower limb and upper limb (31.5% and 17.3%, respectively). In their study, orthopedic fractures in multiple anatomic areas were present in 23.6% of patients. Men were more likely to suffer from femur fractures than women, who were more likely to suffer from humerus fractures (15). The types of fractures sustained in RTAs vary per Saudi Arabian region. Sonbol et al. (19) noted that in the western region, male patients were more likely to sustain tibial and patellar fractures, whereas female patients were more likely to sustain distal femoral fractures. According to their findings, the neck and tibia were the most important factors for the age group (19). The femoral bone is the strongest in the body, and the amount of energy needed to break it is usually high, especially in young patients, which explains the high incidence of associated injuries (23). Those associated injuries can be life-threatening, limb-threatening, or have long-term sequelae if not discovered or treated early, such as femoral neck fracture in young patients. Middle shaft femoral fracture is more common, especially in young men, and it is more common on the right side. These fractures tend to occur more frequently in the younger age group, which is also the age group when reckless driving is most prevalent (27).
As per Almansouf et al. (21), femoral fractures were the most often detected kind of lower limb fracture following MVAs (31.5%), and multiple lower limb fractures were mostly observed in pedestrians who were involved in road accidents. Another included study in this review analyzed the prevalence of injuries associated with femoral shaft fractures after RTAs in children and found that 29.1%, whereas isolated FSFs were 70.9% (20). Bilateral femoral fractures were more prevalent among children aged 10 years or more (12.3% vs. 6.7%), whereas tibial fractures were more common among younger children (4.0% vs. 3.5%). The World Health Organization looked at 13–15-year-olds in 26 countries who had sustained injuries due to RTAs, which showed that 10% of them had sustained a minor head injury and 37% had sustained a fractured limb (20).
In Saudi Arabia, maxillofacial fractures and facial injuries are most frequently caused by MVAs. The orbit (32%), located in the midface (64%), was the most often fractured area. The subcondylar fracture location made for 19% of all mandibular fractures. Moreover, half of the patients sought out conservative therapy in a study that investigated maxillofacial fractures resulting from MVAs(6). Failure to wear seatbelts, airbag deployment, and the face hitting the steering wheel are possible explanations for this finding. However, in other international studies, the causes of maxillofacial fractures and other fractures varied. MVAs appears to be more prevalent in low-to-middle-income Asian and African nations and less prevalent in developed nations like Australia, the United States, and the United Kingdom, where there is increased awareness of the use of protective measures like mandatory seat belt use and advancements in airbag technology. This may be due to the different geographic regions and socioeconomic status of the populations studied (28).
Alotaibi et al. (9) showed that single fractures were more common than multiple fractures. However, a larger percentage of bilateral and multiple-site fractures, mostly in the head and neck regions, was reported by Aloudah et al. (15) and Sonbol et al. (19). The patterns of RTA-related bone injuries or fractures reported in other countries were comparable to those in the Saudi Arabian regions (29), and this significantly warrants further research into promoting change in RTA-related injuries and fractures. According to one of the papers considered in this analysis, 73% of victims suffered multiple fractures in the lower limb site. Additionally, it described the mechanism of fractures, demonstrating that motor vehicle accidents (41%) and motorcycle accidents (9%), respectively, also pedestrians suffered the majority (50%) of multiple lower limb fractures. The most frequently broken bone in motor vehicle accidents was the femur (47.2%), while the most frequently broken bone in pedestrian accidents (37.1%) and motorbike accidents (24.4%) was the tibia (21).
Accidents occurred in 30.8% of the instances in the morning, 18.5% in the evening, and 50% during the afternoon rush hour. Additionally, it was shown that night accident accounted for 27.1% of all RTA cases, while simple fractures made up 56.4% of cases in the afternoon and complex fractures made up 54.2% of cases in the morning. During the afternoon, about 46% of individuals with RTA had open fractures (9). In Saudi Arabia, the daytime is the traditional time for working in institutions, schools, and public and private offices. As a result, there are many vehicles on the road during this period. There are also many vehicles between 6 and 9 PM, which is when people are returning from work, going out for entertainment, shopping, or attending to family or religious obligations. As a result, there are a lot more automobiles on the road during this rush hour. According to other studies, this corresponds to the time when individuals are enjoying outdoor leisure activities.
The severity of injury and hospitalization
In terms of severity, AlHammad (5) showed an accident-to-death ratio of 20:1, which was quite similar to another study carried out in Saudi Arabia (32:1) and remarkably different than the ratio in the USA of 283:1 (1). Altoibi et al. (9) investigation showed a sizeable number of complicated fractures (10.2%), of which 50% occurred in the lower limbs and approximately 30% in the upper limbs. The lower limbs (64.3%) had the highest prevalence of open fractures, while the upper limbs (32.1% of the cases) had the lowest. Almost half of the MVA victims required Intensive Care Unit (ICU) admission. The GCS scores of our subjects showed a mean of 11.34 on admission. Most GCS scores fell in the mild range (6). Almansouf et al. (21) studied the length of stay in lower limb fractures and discovered that patients who had been in car accidents had a longer hospitalization period because they needed an open surgery that required more extensive intervention, whereas pedestrian and motorcycle accidents had a mean shorter duration than car accidents.
To the best of our knowledge, this is the first systematic review to analyze the fracture pattern due to RTAs in Saudi Arabia. However, this systematic review is limited by several factors initially, most studies included only admitted patients; therefore, non-admitted minor fractures or those who died before reaching the hospital were not captured. Not all the studies reported some essential information regarding the nature of the accidents, type of vehicle, positions inside the vehicle, and the circumstances of the passengers during them that could have provided more insight into the problem and helped formulate plans to combat it.
Conclusion
Lower limb fractures, especially femur bone fractures, are prevalent in Saudi Arabia, and caused by RTAs, especially among young males. Therefore, the concerned authorities need to employ and implement stricter traffic rules to minimize the risk of RTA fractures and their subsequent increased morbidity and mortality rates.
Disclosure
Conflict of interest
There is no conflict of interest
Funding
No funding
Ethical consideration
Non applicable
Data availability
Data that support the findings of this study are embedded within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.
