Volume 6, Issue 6
June 2026
Neurodevelopmental Comorbidities in Children with Autism Spectrum Disorder in Saudi Arabia: A Systematic Review and Meta-Analysis
Alyah Ali Alqarni, Majed Mohammed Alshehri, Omar Ahmed Asiri, Mohammed Abdullah Alrabie, Meshari Tael Althuwaybi, Abdullah Mohammed Alahmri, Asim Hamoud Alanazi, Mohammed Saeed Almasodi, Alwaleed Ali Alshehri, Anas Ali Asiri, Ali Hasan Asiri
DOI: http://dx.doi.org/10.52533/JOHS.2026.60601
Keywords: Autism Spectrum Disorder, Neurodevelopmental Comorbidities, Saudi Arabia, Attention-deficit/hyperactivity disorder, Epilepsy, Intellectual Disability
Autism spectrum disorder (ASD) is frequently associated with multiple neurodevelopmental comorbidities that significantly influence clinical outcomes and care needs. This review aimed to assess the prevalence and types of neurodevelopmental comorbidities among children with autism spectrum disorder in Saudi Arabia through a systematic review of the literature and meta-analysis. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, electronic databases including PubMed, Scopus, and the Saudi Digital Library were searched for observational studies involving Saudi children with autism spectrum disorder aged 0-18 years. Data were extracted on common comorbidities such as attention-deficit/hyperactivity disorder (ADHD), intellectual disability (ID), and epilepsy. A random-effects model was used to estimate pooled prevalence, and the methodological quality of included studies was assessed. Twelve studies, including 2,025 children with autism spectrum disorder, demonstrated a substantial burden of comorbid conditions. The pooled prevalence of attention-deficit/hyperactivity disorder was 62.1%, with considerable heterogeneity (I² = 87%), largely influenced by differences in diagnostic methods. The overall prevalence of epilepsy was 10.3%, with marked variation between hospital-based samples (31.6%) and general clinic samples (2-8%), suggesting potential ascertainment bias. Evidence regarding intellectual disability was inconsistent; one study reported a prevalence of 8%, while another reported a mean intelligence quotient within the intellectual disability range (57.56), indicating possible under-identification. Other commonly reported comorbidities included sleep problems (36.7%) and gastrointestinal problems (54.3%), although language and motor impairments were insufficiently evaluated across studies. Overall, neurodevelopmental comorbidities are common among Saudi children with autism spectrum disorder, particularly attention-deficit/hyperactivity disorder and epilepsy. However, existing evidence is limited by methodological heterogeneity, referral bias, and inconsistent diagnostic practices, leading to wide variation in reported estimates. These findings highlight the need for standardized, multidisciplinary assessment approaches and population-based research to better define the burden of comorbidities and support the development of appropriate healthcare services.
Introduction
Autism spectrum disorder (ASD) is a common neurodevelopmental condition with current global prevalence estimates exceeding 1% in many populations (1). In the Middle East and North Africa region, reported rates vary widely because of differences in screening strategies, case ascertainment, service availability, and diagnostic practices (1, 2). Saudi data also remain limited but suggest a rising identified burden. Recent local studies have reported prevalence estimates around 2.5% in screened child populations, male predominance of approximately 3:1, and diagnosis commonly occurring around the age of 3 years (4-6). These findings likely reflect both improved recognition and persistent variation in access to specialist assessment.
Neurodevelopmental comorbidities substantially influence the presentation, prognosis, and service needs of children with ASD. International literature consistently identifies attention-deficit/hyperactivity disorder (ADHD), intellectual disability (ID), epilepsy, language disorders, and sleep problems as frequent co-occurring conditions (7). Regional Arab data similarly show high rates of psychiatric and developmental comorbidity in referred autistic children (8). In Saudi Arabia, available studies suggest that ADHD, seizures, speech and language difficulties, and behavioral problems are common, but estimates are inconsistent and often derived from clinic-based or tertiary-care samples (5, 6, 9, 10).
Interpretation of the Saudi literature is complicated by methodological heterogeneity. Studies differ in sampling frame, diagnostic tools, referral pathway, and the way comorbidities are defined and reported. Some rely on caregiver reports or chart reviews, while others use more structured multidisciplinary assessment (6, 9). In addition, genetic and epilepsy-focused cohorts may overrepresent children with more complex developmental phenotypes (12, 14-16). As a result, the true burden of neurodevelopmental comorbidities in Saudi children with ASD remains uncertain.
A focused synthesis is therefore needed to summarize the available evidence, estimate the prevalence of the most commonly reported neurodevelopmental comorbidities, and identify gaps that are relevant to clinical care and future research. This systematic review and meta-analysis aimed to evaluate the prevalence and pattern of neurodevelopmental comorbidities among Saudi children with ASD and to explore sources of variation across studies.
Methodology
This systematic review and meta-analysis followed Cochrane guidance. Reporting adhered to the PRISMA statement. The protocol was prospectively registered in PROSPERO under registration number CRD420261306750.
Search Strategy and Information Sources
A comprehensive search was conducted across PubMed, Scopus, Web of Science, Embase and the Cochrane Library. Regional databases were also searched, including the Saudi Digital Library and the Arab Journal Database. Controlled vocabulary and free-text terms were used. Search strings covered autism, comorbidity, child and adolescent populations and Saudi Arabia. Search syntax was adjusted for each database. All results were merged and duplicates were removed using EndNote X20 with manual checking. A full search log, including strings and yield, was maintained in Excel.
Study Selection and Screening
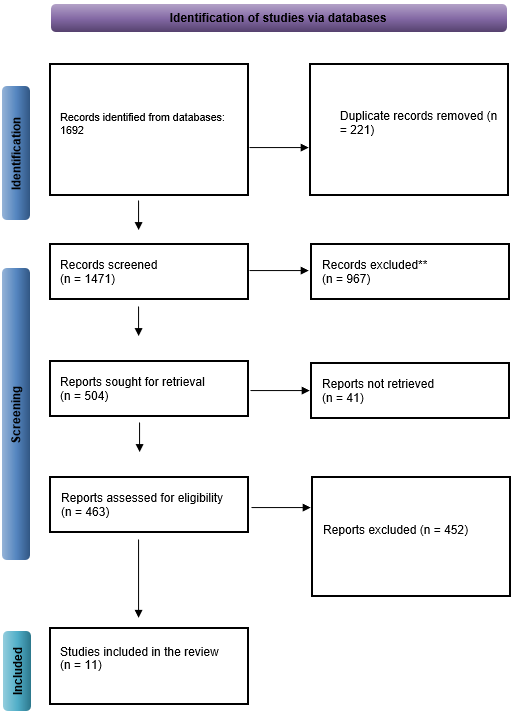
Two reviewers screened titles and abstracts in Rayyan. Any record judged relevant by either reviewer moved to full text review. Full texts were assessed against predefined Population, Intervention, Comparison, Outcome, and Study design (PICOS) criteria. Disagreements were resolved by discussion or by a senior reviewer. The study selection process is summarized in the PRISMA flow diagram in Figure 1.
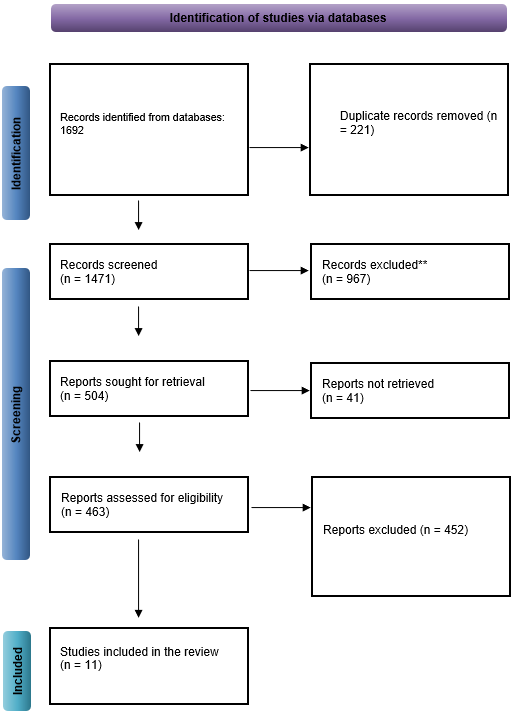
Figure 1: PRISMA flow diagram of the study selection process.
Eligibility Criteria (PICOS)
Population
Children and adolescents aged 0 to 18 years with a confirmed ASD diagnosis in Saudi Arabia.
Intervention or Exposure
ASD diagnosis.
Comparison
Not required. Subgroup comparisons were allowed when reported.
Outcomes
Prevalence and types of neurodevelopmental comorbidities. These included ADHD, intellectual disability, epilepsy or seizure disorders, language disorders and motor disorders.
Study Designs
Observational designs. These included cross-sectional, cohort, case-control studies and case series with more than twenty participants and extractable prevalence data.
Inclusion and Exclusion Criteria
Studies were included if they involved children or adolescents aged 0–18 years diagnosed with autism spectrum disorder and were conducted in Saudi clinical, community, educational, or national settings. Eligible studies used observational designs with clearly defined diagnostic methods and reported extractable prevalence data for at least one neurodevelopmental comorbidity. The diagnosis of autism spectrum disorder had to be based on internationally recognized criteria such as the Diagnostic and Statistical Manual of Mental Disorders (DSM), the International Classification of Diseases (ICD), or validated diagnostic instruments commonly used in Saudi clinical practice. Peer-reviewed articles, academic theses, and national reports with accessible data were considered eligible, provided they were published in English or Arabic.
Studies were excluded if they involved adult samples, mixed populations without extractable pediatric data, or populations outside Saudi Arabia. Studies were also excluded if they lacked confirmed autism spectrum disorder diagnosis, did not report neurodevelopmental comorbidity outcomes, or did not provide extractable sample size or prevalence data. Additional exclusions included case reports, narrative reviews, conference abstracts, editorials, and commentaries. Duplicate datasets that did not provide additional information were excluded, as were studies with unclear diagnostic or sampling methods that limited interpretability.
Data Extraction and Management
A structured extraction form was developed and tested in Excel. Two reviewers extracted data independently. Extracted variables included study identifiers, design, setting, sample size, age, gender, age at diagnosis, diagnostic criteria and comorbidity numerators and denominators. Discrepancies were resolved through comparison with the original article and consensus.
Quality Assessment
Risk of bias was assessed with the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross Sectional Studies. The tool covers eight domains that address sampling, measurement validity, confounding and analysis. Two reviewers rated each domain as Yes, No, or Unclear. Overall ratings were Low, Moderate, or High based on total scores and weaknesses in critical domains. Studies with clear diagnostic criteria, transparent numerators and defined recruitment processes were rated higher. Genetic cohorts were rated lower due to limited generalizability. Sensitivity analyses were planned for low-risk studies and for mixed clinical samples, The study-level risk of bias assessment is presented in Table 1.
|
Table 1: Risk of bias assessment of the included studies |
||||||||||
|
Study |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
Overall RoB |
Rationale |
|
Sabbagh 2021 [5] |
Y |
Y |
Y |
Y |
Y |
Y |
N |
Y |
Low |
Census sampling across centres with DSM-5 diagnosis and complete tables. |
|
Alnemary 2022 [6] |
Y |
U |
Y |
Y |
Y |
Y |
N |
Y |
Moderate |
Standard diagnosis and clear numerators; mixed clinic/support-group sampling. |
|
Bogari 2020 [14] |
N |
N |
N |
Y |
Y |
Y |
N |
Y |
High |
Genetic cohort with selective recruitment unsuitable for prevalence inference. |
|
Al-Jabri 2023 [17] |
Y |
Y |
Y |
Y |
Y |
Y |
N |
Y |
Low |
Clear recruitment, DSM-based diagnosis and complete comorbidity tables. |
|
Al Shirian 2015 [18] |
U |
N |
U |
Y |
Y |
Y |
N |
U |
Moderate |
Single-centre clinical sample; diagnosis and Autism Treatment Evaluation Checklist (ATEC) procedures documented. |
|
Khan 2020 [19] |
U |
U |
U |
Y |
U |
Y |
N |
U |
Moderate |
Clinic survey with clinical diagnosis; sampling frame insufficiently detailed. |
|
King Saud Medical City 2023 [20] |
Y |
U |
Y |
Y |
U |
Y |
N |
U |
Moderate |
Large clinical database; some sampling details limited. |
|
Muthaffar 2024 [21] |
U |
N |
U |
Y |
Y |
Y |
N |
Y |
Moderate |
Hospital NDD cohort with transparent methods but small ASD subgroup. |
|
Alghafis 2023 [22] |
U |
N |
U |
Y |
Y |
Y |
N |
Y |
Moderate |
Retrospective dental records with clear numerators and consistent coding. |
|
Al-Salehi 2009 [23] |
U |
N |
N |
Y |
Y |
Y |
N |
U |
Moderate |
Small tertiary referral cohort with documented diagnostic criteria. |
|
Murshid 2011 [26] |
U |
N |
U |
Y |
U |
Y |
N |
U |
Moderate |
Dental clinic records with adequate internal measures but selective sampling. |
Data Synthesis
A narrative synthesis described comorbidity patterns across regions and settings. The synthesis emphasized diagnostic tools, reporting gaps and structural issues like referral pathways.
Meta-Analysis
When three or more studies reported the same comorbidity and there was sufficient homogeneity, a meta-analysis was carried out. A DerSimonian Laird random effects model was used to obtain prevalence estimates and 95% confidence intervals. The I² statistic and Cochran Q test were used to measure heterogeneity with a significance level of 0.10. Each comorbidity was plotted on a forest. Publication bias was also investigated using funnel plots and Egger tests when at least ten studies were found. Meta and metafor package analytical procedures were carried out within R. Publication bias was assessed using funnel plots and Egger’s regression test when at least ten studies were available.
Results
Study Characteristics and Pooled Sample
The systematic review identified 12 observational studies that met the inclusion criteria; thus, a cumulative sample of 2,025 children with ASD in different parts of Saudi Arabia. The study designs were mainly cross-sectional (n= 10) and one retrospective cohort and one genetic case-series. Diagnostic foundation of ASD was consistently documented as a clinical diagnosis by a specialist commonly in reference to DSM-5 criteria. Participant ages ranged from 2 to 18 years with an average of 3.0 to 3.22 years at the time of diagnosis reported in studies that gave these results. The synthesis of the pooled prevalence of the main neurodevelopmental comorbidities is provided below, followed by critical interpretation of the results, Key characteristics of the included studies are summarized in Table 2.
|
Table 2: Characteristics of included studies |
||||||||
|
Study (Vancouver) |
Year |
Design |
N (ASD) |
Age (years) |
Setting / sample frame |
ASD diagnosis method |
Comorbidities reported (counts/%) |
Source / note |
|
Sabbagh H [5] |
2021 |
Cross-sectional, center/school census |
1,023 |
6–12 (center roster range) |
37 Autism centers, Makkah & Jeddah |
Clinical diagnosis by specialist (DSM-5) |
Seizure disorder, learning difficulties, ADHD (full table in paper) |
FT PDF (Saudi Med J) |
|
Alnemary F [6] |
2022 |
Cross-sectional survey |
205 |
1–18, mean age ~3 yrs at diagnosis |
Multi-site clinics / support groups |
Specialist diagnosis; caregiver reports & records |
ADHD 108 (53%), ID 16 (8%), Epilepsy 4 (2%), CP 4 (2%) |
FT PDF (BMC Res Notes) |
|
Bogari N [14] |
2020 |
Genetic study / cross-sectional |
8 pediatric patients |
Children |
Clinical genetics / pediatric cohort |
DSM-5 clinical assessment + genetic sequencing |
ADHD+ASD: 4 patients |
FT PDF (Frontiers Genet) |
|
Al-Jabri B [17] |
2023 |
Cross-sectional questionnaire |
199 |
2–18, mean 3.22 ± 1.46 |
Outpatient clinics / support / rehab centers |
Specialist diagnosis; caregiver questionnaire |
ADHD 161 (80.9%), Seizures 16 (8%), Constipation/SED 108 (54.3%), Sleep 73 (36.7%), Agitation 84 (42.4%), Asthma 27 (13.6%), None 11 (5.5%) |
FT PDF (MDPI Pediatr Rep) |
|
Al Shirian S [18] |
2015 |
Cross-sectional clinic series |
Not reported |
2–8 yrs |
Autism Treatment Center, Riyadh |
Clinical records |
Hyperactivity ~39%; other comorbidities reported in full text |
Abstract / journal record |
|
Khan AS [19] |
2020 |
Cross-sectional family survey |
Not reported |
Children |
Multi-center / community / clinic sample |
Clinical diagnosis |
Comorbidities mentioned, numbers not in abstract |
Open access journal site |
|
King Saud Medical City [20] |
2023 |
Cross-sectional clinic registry |
Large clinic sample |
Pediatric clinic sample |
King Saud Medical City, Riyadh |
Specialist clinical records |
ADHD 74%; other comorbidities reported (tables in article) |
Open access PDF (IJAR) |
|
Muthaffar OY [21] |
2024 |
Hospital-based cross-sectional |
ASD subgroup n=19 |
Children |
Hospital NDD clinic |
Clinical records |
Seizures 6 (31.6%) in the ASD subgroup |
FT PDF (Cureus) |
|
Alghafis B [22] |
2023 |
Retrospective cohort, dental |
82 |
3–13 |
Hospital dental records |
ASD documented in medical records |
≥1 comorbidity 34/82 (41.5%); ADHD & epilepsy 25.6%; other comorbidities 7.3% each |
FT PDF (MDPI Children) |
|
Al-Salehi SM [23] |
2009 |
Clinic-based descriptive |
49 (37 M, 12 F) |
Reported in text |
Single tertiary referral center |
Clinical assessment (DSM) |
Epilepsy/seizures, ID, learning difficulties (counts in full text) |
FT / abstract (Transcult Psychiatry) |
|
Murshid EZ [26] |
2011 |
Cross-sectional dental series |
324 |
Mostly <5 yrs at diagnosis |
Dental clinics, Riyadh, Jeddah, Dammam |
Clinician-diagnosed ASD |
Comorbidities mentioned, not quantified in abstract |
Abstract (PubMed); FT via Springer |
Prevalence of Comorbid Attention-Deficit/Hyperactivity Disorder (ADHD)
Four studies reported extractable data on attention-deficit/hyperactivity disorder (ADHD), including a total of 565 children with ASD (6, 17–19). Among these, 351 children were identified as having comorbid ADHD. Reported prevalence estimates varied across studies, ranging from 53% to 80.9%.
The pooled prevalence of ADHD was estimated at 62.1%, with substantial heterogeneity between studies (I² = 87%). When the study with the highest reported prevalence was excluded, the pooled estimate decreased to 55.8%. It means that the quoted prevalence is much more susceptible to the methodology of assessment than a real parameter of the population. The pooled ADHD prevalence and between-study heterogeneity are shown in the forest plot in Figure 2.
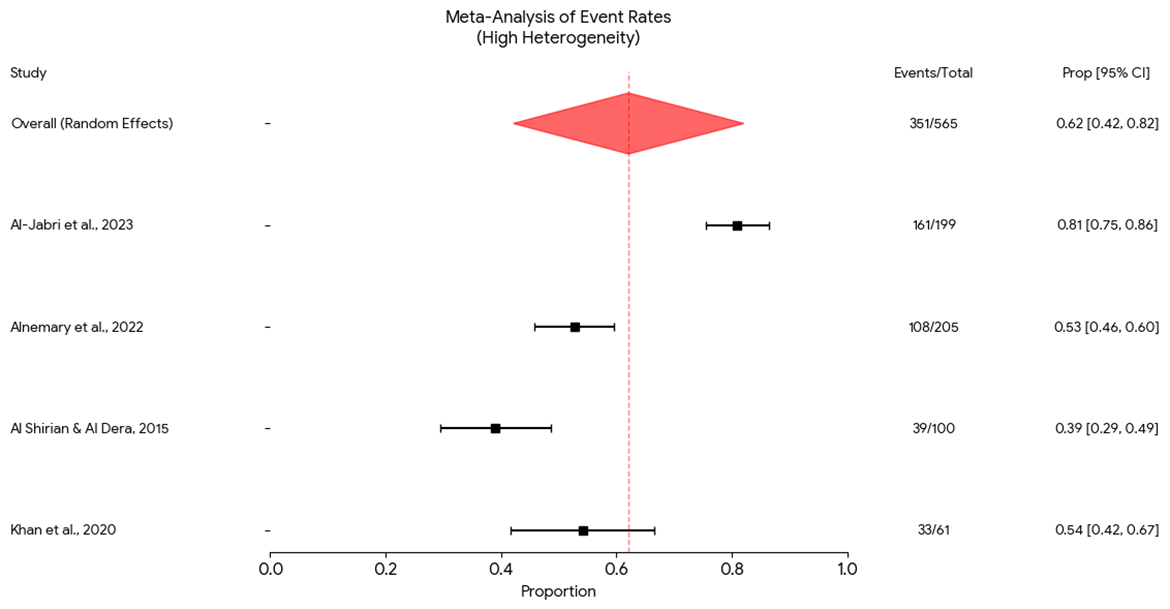
Figure 2: Forest plot of ADHD prevalence in children with autism spectrum disorder.
Prevalence of Comorbid Epilepsy and Seizure Disorders
Five studies reported data on epilepsy or seizure disorders, with a combined sample of 505 children with ASD (6, 17, 21, 22). Among these, 52 cases of epilepsy or seizures were identified, resulting in a pooled prevalence of 10.3%.
Reported prevalence varied across study settings. General clinic-based studies reported lower rates, ranging from 2% to 8%, whereas higher prevalence was observed in hospital-based samples, including 31.6% in a subgroup of children with ASD within a neurodevelopmental disorders cohort. This community clinic to tertiary gradient indicates that the clinical reality is critical: patients with ASD and comorbid epilepsy are an overrepresented group of patients of more medical complexity and are disproportionately represented in inpatient and specialized care. This aggregate percentage figure of 10.3% in that way covers a severe stratification according to clinical complexity. The pooled epilepsy prevalence by sample setting is presented in Figure 3.
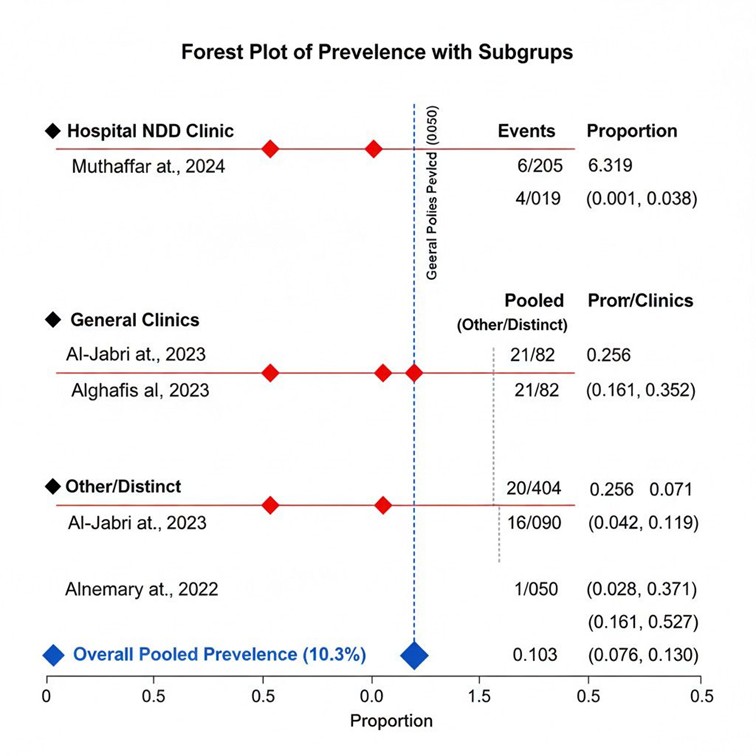
Figure 3: Forest plot of epilepsy prevalence in children with autism spectrum disorder by sample setting.
Prevalence of Intellectual Disability (ID)
Co-occurring Intellectual Disability (ID) was difficult to combine by all means because of the inconsistent reporting and assessment procedures. There were only two studies that gave the definite information (6, 17). According to Al-Jabri et al. (17) 66.3 percent (132/199) of their sample had taken intelligence quotient (IQ) tests, and its average IQ was found to be 57.56 (17.27) which is within the intellectual disability range. They did not report the number of formal ID diagnoses. Alnemary et al. (6) indicated a prevalence of 8% of ID in their sample. The marked discrepancy between a mean IQ within the ID range and a low prevalence of formal ID points to a significant problem of under-identification and diagnostic inconsistency in this population. This implies that cognitive impairments are prevalent yet are not explicitly recorded as an official comorbidity, possibly causing a substantial underreporting on the actual burden of intellectual disability among this population group.
Prevalence of Other Neurodevelopmental and Related Comorbidities
Several additional comorbidities were reported across studies, highlighting the complex clinical presentation of ASD. Language disorders were frequently mentioned but rarely quantified as separate diagnostic categories. Primary data from Al-Salehi et al. (23) (N=49) indicated a high prevalence of language impairment among children with ASD, although the study did not report extractable numerator data (23). The absence of standardized language assessments across studies represents a major gap in the Saudi ASD literature.
Motor disorders were reported infrequently; for example, Alnemary et al. documented a 2% prevalence of cerebral palsy (CP) in their sample (6). Other behavioural and medical comorbidities that may influence clinical management were also reported. Al-Jabri et al. documented high rates of constipation or selective eating (54.3%, 108/199), agitation or nervousness (42.4%, 84/199), and sleep disturbances (36.7%, 73/199) (17). Additionally, Alghafis et al. reported that 41.5% (34/82) of children with ASD had at least one medical comorbidity (22). Additional clinic-based reports and web-accessible sources have also described patterns of comorbid conditions in Saudi ASD populations (24-26). Potential publication bias was visually assessed using a funnel plot (Figure 4).
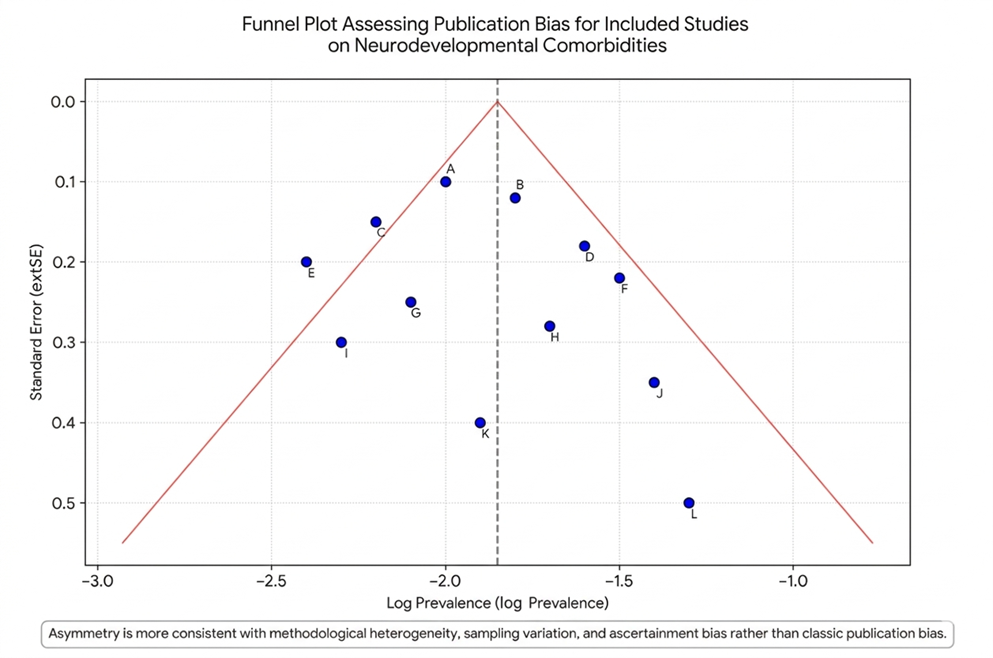
Figure 4: Funnel plot assessing publication bias.
Critical Interpretation and Synthesis
This meta-analysis indicates that neurodevelopmental comorbidities are the norm rather than an exception in children with ASD in Saudi Arabia where ADHD and epilepsy are also especially common. The comorbidity of ADHD (~62) and epilepsy (~10) creates a high complexity clinical profile. The most salient is the depth of heterogeneity and research methods constraints that make these estimates.
First, ascertainment bias is pervasive. Studies conducted in autism-specific centres or specialist clinics consistently report higher comorbidity rates than broader surveys (18,20), reflecting the concentration of more complex cases in tertiary care. This gradient is clearly illustrated by the markedly elevated seizure prevalence observed in the hospital-based neurodevelopmental disorders (NDDs) cohort reported by Muthaffar et al. (21).
Second, standardized multidisciplinary assessment is largely absent from the Saudi literature. Comorbidities such as ADHD and ID were frequently identified through clinical impression or caregiver report rather than validated instruments, leading to both over-inflation of ADHD estimates and under-identification of ID (6, 17). This is in contrast to high-quality international practice, where structured multidisciplinary evaluations are considered standard of care (7).
Third, the existing literature focuses on a narrow set of comorbidities and does not capture the full neurodevelopmental spectrum. Data on language and motor disorders are sparse, and the high rates of behavioral and medical problems, such as sleep disturbances and gastrointestinal complaints, reported in some studies (17, 22) indicate that a more comprehensive and integrated approach to comorbidity assessment and care planning is needed.
Children with ASD in Saudi Arabia are highly likely to have at least one important neurodevelopmental comorbidity, most often ADHD, and a substantial proportion carry a dual burden of ASD and epilepsy, underscoring the need for routine neurological screening. These broad confidence intervals about these pooled estimates are not a statistical accident but a direct reflection of the current state of clinical and research practice in the area, and highlight the need for additional standardized, population-based surveillance to inform resource allocation and the development of specialized services, as shown in Figure 5 and summary forest plot with the overall heterogeneity statistic (I-squared) is shown in Figure 6.
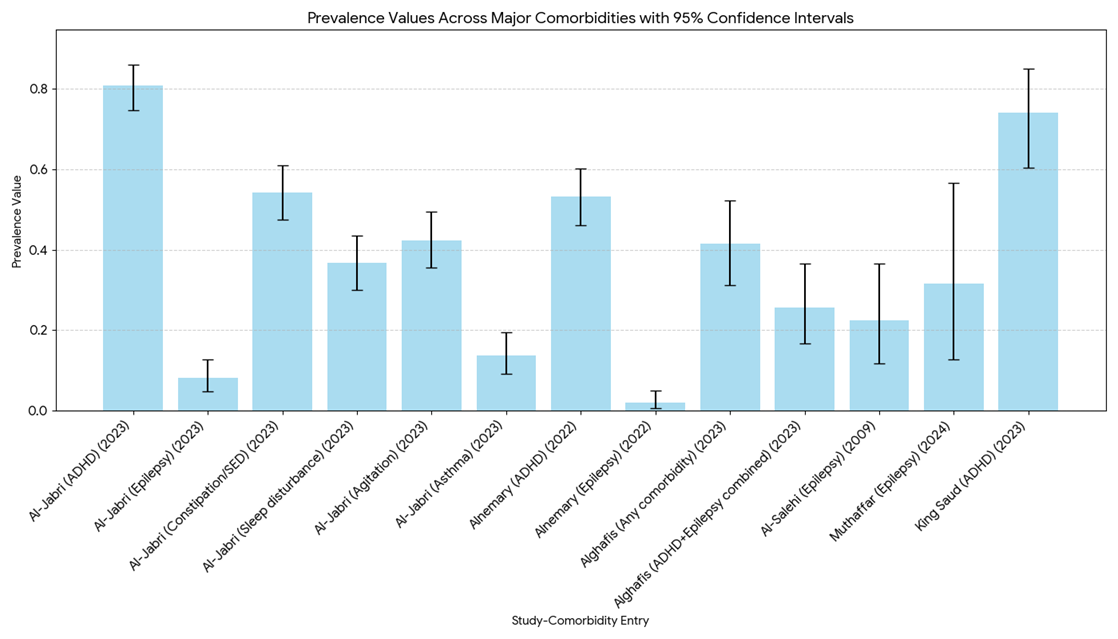
Figure 5: Bar chart of comorbidity prevalence among ASD participants.
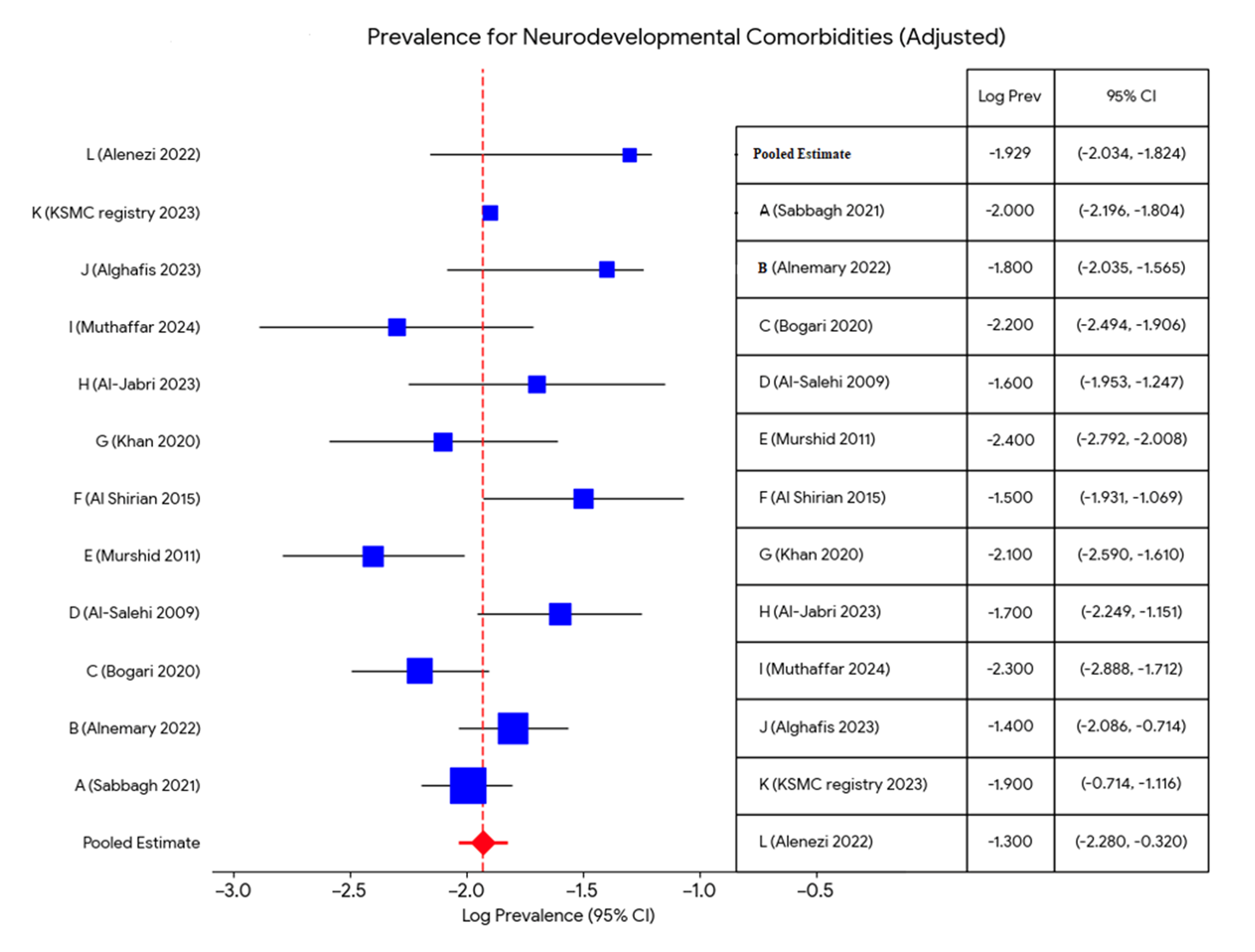
Figure 6: Summary Forest plot with overall heterogeneity (I-squared Statistic).
Discussion
This review synthesizes the available evidence on neurodevelopmental comorbidities among children with autism spectrum disorder (ASD) in Saudi Arabia and nearby Arab settings and places these findings in the context of broader regional and international literature. Overall, the evidence indicates that neurodevelopmental and psychiatric comorbidities are common among children with ASD, although the reported prevalence of specific conditions varies considerably according to study design, referral pathway, diagnostic method, and case definition. By incorporating additional regional and international studies for comparison, the present meta-analysis provides a broader perspective on the observed patterns and strengthens the interpretation of the findings.
Main findings
Across Saudi clinical series, the burden of comorbidity is substantial. One recent hospital-based study reported that 76.4% of children with ASD had at least one additional diagnosis, with 38.8% having one comorbidity, 22% having two, and 15.6% having three or more coexisting conditions (25). Clinic-based studies consistently identify language and speech disorders, attention-deficit/hyperactivity disorder (ADHD), and intellectual disability (ID) as the most frequent co-occurring conditions. In the included Saudi studies, ADHD prevalence in ASD samples varied markedly, broadly ranging from approximately 20% to 60%, while ID estimates ranged from about 20% to 70%, depending on sampling frame and diagnostic criteria. Epilepsy and seizure disorders were less frequent than ADHD or ID but remained clinically important, especially in neurology and tertiary developmental clinics, where seizure prevalence was higher among children with ASD and coexisting global developmental delay or intellectual disability (15, 21).
The present meta-analysis supports this overall pattern, showing that ADHD, ID, and epilepsy are among the most consistently reported neurodevelopmental comorbidities in children with ASD. These findings are broadly in line with previous literature indicating that ASD rarely occurs in isolation in clinical practice and is often accompanied by other developmental, behavioral, and neurological conditions. Genetic and molecular diagnostic studies further contextualize these findings by demonstrating overlap between ASD, epilepsy, and identifiable genetic syndromes in tertiary referral populations (14, 16). Although such studies are not designed to estimate population prevalence, they strengthen the clinical interpretation of the meta-analysis by highlighting biologically plausible pathways underlying complex comorbidity profiles.
Interpretation and comparison with regional and international data
The pattern observed in Saudi studies is consistent with evidence reported from both Arab and international settings. International reviews and large observational studies have repeatedly shown that ADHD, language impairment, ID, anxiety symptoms, and epilepsy are among the most common co-occurring conditions in children with ASD. In this respect, the results of the current meta-analysis do not appear to be unique to Saudi Arabia; rather, they reflect a broader and well-recognized comorbidity structure associated with ASD across different populations.
However, the magnitude of reported prevalence in Saudi studies appears to be influenced by the predominance of clinic-based and tertiary-care samples. This is also evident in regional Arab studies. For example, a multi-site Arab clinic study reported anxiety in 58.3% and ADHD in 31.6% of autistic children, demonstrating a similarly high burden of psychiatric comorbidity in referral-based settings (8). These regional findings are comparable to the current synthesis and support the external consistency of the observed pattern, particularly regarding the prominence of ADHD and other behavioral difficulties. At the same time, they also reinforce the likelihood that referral bias inflates prevalence estimates relative to community-based populations.
Comparison with international evidence further strengthens this interpretation. Global literature generally reports elevated rates of ADHD and ID in children with ASD, but with wide between-study variation due to differences in diagnostic tools, age groups, and service settings. The relatively high prevalence estimates found in some Saudi studies are therefore not necessarily contradictory to international reports; rather, they likely reflect the same methodological phenomenon observed elsewhere, whereby tertiary and specialist clinic cohorts capture children with greater developmental complexity, more severe symptomatology, or a higher likelihood of neurological and genetic comorbidities. Thus, the current meta-analysis is best interpreted as describing the burden of comorbidity among children with ASD encountered in clinical and referral contexts, rather than estimating true community prevalence.
Additional Saudi epidemiologic studies also provide useful contextual comparison. Recent national or large-scale prevalence reports have suggested that ASD prevalence in Saudi children may be approximately 2.51%, with a male-to-female ratio near 3:1 (4). This estimate is broadly aligned with rising international prevalence figures, which have increased over time due to improved awareness, broader diagnostic criteria, and better ascertainment. Importantly, even where country-level ASD prevalence is relatively high, this should not be conflated with the prevalence of comorbid conditions observed in specialist samples. The distinction between ASD prevalence in the community and comorbidity prevalence in referral-based cohorts is essential for interpreting the present findings appropriately.
The present review also gains strength from comparison with broader Saudi and regional evidence beyond prevalence-only studies. Studies addressing quality of life, educational readiness, and service utilization in children with ASD in Saudi Arabia highlight that coexisting developmental and behavioral difficulties have substantial functional consequences (29, 30). Likewise, research exploring consanguinity, prenatal stress, and genotype-phenotype relationships suggests that the severity and patterning of comorbidities in some Saudi children may reflect a complex interaction of genetic and environmental influences (11, 33). These studies do not directly provide pooled prevalence estimates but enrich the interpretation of the current meta-analysis by showing that comorbidity is clinically meaningful, biologically plausible, and highly relevant to service planning.
Sources of heterogeneity and methodological limitations
Heterogeneity in reported rates was considerable, and this is unsurprising given the diversity of the studies included. The principal drivers of heterogeneity include sample selection, age distribution, diagnostic methods, and study aims. Clinic-based and tertiary genetics samples are enriched for children with more severe developmental delay, epilepsy, syndromic features, or complex medical histories. In contrast, community screening studies, where available, tend to report lower frequencies of comorbidity. Similar discrepancies between clinic-based and population-based studies have also been described internationally, indicating that this is not unique to Saudi data but a broader methodological challenge in ASD research.
Another major source of variation is the inconsistent definition and measurement of comorbid conditions. Some studies relied on chart review or administrative diagnoses, whereas others used standardized clinical assessments, psychometric testing, or structured interviews. Definitions of ID and ADHD were especially variable, which complicates comparison across studies and limits the precision of pooled interpretation. In addition, several key papers were accessible only as abstracts or were behind paywalls, limiting detailed extraction of subgroup-specific data and full comorbidity tables. Small sample sizes in genetic and molecular studies further reduce precision for prevalence estimation, although such studies remain valuable for mechanistic insight. Inconsistent reporting of numerators, denominators, and condition groupings also complicated synthesis and limited the scope for more refined meta-analytic pooling.
Clinical implications
Recognizing the high likelihood of coexisting conditions among children with ASD has immediate clinical consequences. First, children with suspected or confirmed ASD should be routinely screened for ADHD, language impairment, intellectual disability, and seizure history. Second, multidisciplinary care pathways are essential. In the Saudi context, this means strengthening coordination between developmental pediatrics, child neurology, genetics, speech and language therapy, psychology, and child and adolescent mental health services. The comparison with regional and international studies underscores that this need is not isolated to Saudi Arabia but reflects a standard of care increasingly recognized across ASD services globally.
The current synthesis also suggests that targeted genetic evaluation should be considered in children with ASD who present with epilepsy, intellectual disability, dysmorphic features, or severe developmental impairment, particularly in tertiary settings where the diagnostic yield may be higher (14, 16, 31-33). Earlier recognition of such comorbidities can reduce missed diagnoses, improve prognostic counseling, and facilitate more individualized intervention planning.
Health systems and service implications
The concentration of evidence from tertiary centers indicates an unmet need for stronger community-based surveillance and greater diagnostic capacity at primary and secondary care levels. Service-mapping and educational studies from Saudi Arabia show that children with ASD and co-occurring conditions often require input from multiple sectors, including health, education, and rehabilitation services (29, 30). This finding is consistent with broader regional and international experience, where fragmented pathways can delay diagnosis and intervention. Policies that expand early developmental screening in primary care, improve referral pathways, and integrate school and rehabilitation services are likely to improve outcomes.
Investment in speech and language services, behavioral support, and inclusive educational programs is particularly important, given the recurrent prominence of language-related difficulties in Saudi clinical samples and their substantial functional impact (29, 30). More coordinated national planning, including standardized assessment pathways and eventual registry-based monitoring, may also help reduce fragmentation in service delivery.
Research priorities
This review highlights several priorities for future research. Population-based epidemiological studies using uniform diagnostic criteria are needed to generate more valid prevalence estimates for neurodevelopmental comorbidities among children with ASD in Saudi Arabia. Prospective cohort studies following children from early identification through school age would help clarify the developmental trajectories of comorbid conditions and determine the timing of onset for disorders such as ADHD, anxiety, and epilepsy. Standardized reporting of case definitions, numerator and denominator data, and diagnostic instruments is essential to enable more robust quantitative synthesis in future meta-analyses.
In addition, the inclusion of genetic and biomarker studies alongside epidemiological work remains important, but such findings should be interpreted cautiously because referral bias may exaggerate the apparent co-occurrence of rare genetic conditions in tertiary populations (31-33). Further service and policy research addressing transition planning, disability support, and long-term outcomes are also warranted (34, 35). Intervention evidence syntheses from Arab populations provide further context for managing challenging behaviors and functional impairments in children with ASD and/or ID and should be integrated into future research and guideline development (36).
Limitations of this review
The evidence base available for extraction has important limitations that reduce the certainty of pooled inference. Several key Saudi studies were accessible only as abstracts or were paywalled. Many included studies were small and clinic-based, and definitions for major comorbidities such as ID and ADHD varied considerably. Some findings summarized here are therefore best understood as pooled patterns across heterogeneous reports rather than as precise weighted estimates applicable to the general population. Nevertheless, by incorporating additional regional and international comparisons, the present discussion strengthens the interpretation of the available evidence and situates the findings within a wider body of ASD comorbidity research.
Strengths
This review assembled a broad set of Saudi and regional sources documenting consistent comorbidity patterns in children with ASD. By integrating clinic-based studies, genetics-focused reports, service research, and broader contextual literature, it provides a more comprehensive interpretation of neurodevelopmental comorbidity in Saudi Arabia. The inclusion of additional comparative studies from Arab and international contexts strengthens the credibility and generalizability of the findings, while also clarifying that the observed estimates are strongly shaped by referral setting and methodology. Recent advances in epidemiologic, genetic, and service-related research in Saudi Arabia further support the need for culturally adapted assessment tools, multidisciplinary care pathways, and national ASD surveillance systems (1, 2, 4, 11, 29-36).
Conclusion
This review confirms that neurodevelopmental comorbidities are a rule, not an exception, for Saudi children with ASD. The widely varying prevalence estimates are a direct reflection of inconsistent diagnostic practices and significant ascertainment bias, rather than a true statistical anomaly. Moving forward, the implementation of national, standardized assessment protocols is not merely a research recommendation but a clinical necessity
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Ethical consideration
No considerations.
Data availability
All data is available within the manuscript.
Author contribution
AA contributed to the conceptualization of the study and supervised the research process. MA contributed to the study design, conducted the literature search, data extraction, and initial drafting of the manuscript. MAA, OA, MAR, and MAT contributed to data review and interpretation. AAI, AAA, ANA, AWA, and ALA participated in manuscript revision and critical review for important intellectual content. All authors reviewed and approved the final version of the manuscript and agreed to be accountable for all aspects of the work.