Volume 6, Issue 5
May 2026
Fulminant Meningococcal Meningitis in a Pregnant Woman with AQP4-Positive Neuromyelitis Optica Receiving Ravulizumab: A Case Report
Shaikha Almheiri, Asma Musa
DOI: http://dx.doi.org/10.52533/JOHS.2026.60502
Keywords: Fulminant Meningococcal Meningitis, Maternal Health, Neuromyelitis optica spectrum disorder, Pregnancy, Neuroimmunology, Neisseria meningitidis
Background: Neuromyelitis optica spectrum disorder (NMOSD) is a recurring autoimmune disease of the central nervous system. Disease management is particularly challenging during pregnancy, as 77% of patients have experienced relapses during the intrapartum and postpartum period. This can be attributed to immunomodulation during pregnancy, which leads to increased disease activity. The pathogenesis involves Aquaporin 4 (AQP4) IgG antibodies binding to astrocytic water channels, initiating complement activation, resulting in astrocyte injury. Complement inhibitors are increasingly used to prevent relapses. Nevertheless, terminal complement blockade is associated with high susceptibility to infections by encapsulated bacteria, particularly Neisseria meningitidis.
Case presentation: We report a case of a 32-year-old pregnant woman at 33+4 weeks’ gestation, who presented to the emergency department with acute fever and confusion. She had a known history of AQP4-IgG-positive NMOSD and received 300 mg ravulizumab every 8 weeks. Blood and cerebrospinal fluid analysis indicated systemic infection. Gram staining revealed Gram-negative diplococci; polymerase chain reaction (PCR) confirmed Neisseria meningitidis infection. Complementary studies revealed complete inhibition of terminal complement. She
Conclusion: This rare case demonstrates the therapeutic dilemma in managing NMOSD during pregnancy. While continuing treatment carries the risk of infection, stopping the drug could potentially lead to a relapse. Further studies are essential to establish safety and clinical guidelines for the management of such autoimmune diseases during pregnancy.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a life-threatening, recurring, inflammatory autoimmune disease of the central nervous system (CNS), which occurs infrequently, with a prevalence ranging from 0.7 to 10 per 100,000 individuals across different populations (1). It was recently identified as a distinct clinical entity from multiple sclerosis, manifesting clinically as optic neuritis, myelitis, and other brain and brainstem-related syndromes. It may be associated with aquaporin 4 (AQP4)-antibody-seropositive autoimmune astrocytopathic disease, myelin oligodendrocyte glycoprotein (MOG)-antibody-seropositive inflammatory demyelinating disease, or double-seronegative disease (2). AQP4-antibody seropositive type is particularly common among females, with a 9:1 ratio compared with males, and a mean age at onset of approximately 40 years (3).
In terms of pathogenesis, NMOSD is mediated by IgG antibodies against AQP4. AQP4 is a water-channel protein highly expressed in the CNS, particularly in astrocyte processes at the blood-brain barrier. They facilitate water movement across the blood-brain barrier (and blood-spinal cord barrier), modulate neuronal excitability, enhance astrocytic migration, and are involved in neuroinflammation. They are also found in the parietal cells of the stomach, the airways, and exocrine glands, and the epithelial cells of the kidney. In this context, the complement system is activated upon binding of IgG antibodies to AQP4 tetramers, leading to lytic damage from the subsequent inflammatory response. While some patients may have a single episode, most require long-term immunotherapy to manage the persistent, relapsing nature of the disease. Complement C5 inhibitors, such as ravulizumab, are increasingly used to prevent relapses (4).
Despite its therapeutic efficacy, terminal complement blockade is associated with high susceptibility to infections by encapsulated bacteria, particularly Neisseria meningitidis. Given that complement-mediated bactericidal activity is a key component of host defense against meningococcal infection, pharmacologic inhibition of C5 markedly increases the risk of invasive meningococcal disease (5). Studies have estimated that patients receiving terminal complement inhibitors may have a 1,000–2,000-fold higher risk of meningococcal infection than the general population, even when appropriate vaccination has been administered. Physiological alterations in both innate and adaptive immune responses during pregnancy are necessary to maintain maternal tolerance to the fetus. However, these immunomodulations modify susceptibility to infections and autoimmune disease. The management of NMOSD during pregnancy poses a complex challenge, requiring careful balancing of maternal disease control against potential maternal and fetal risks associated with immunosuppressive therapies (6, 7).
Of greater concern, monoclonal antibodies targeting complement pathways may cross the placenta during the second and third trimesters via Fc receptor–mediated transport; fetal exposure to these agents may theoretically influence neonatal immune function, particularly components of the complement system essential for defense against encapsulated organisms (8). Nevertheless, clinical data regarding the safety of complement inhibitors during pregnancy are limited. Hereby, we report a rare case of fulminant meningococcal meningitis occurring during late pregnancy in a patient with AQP4-positive NMOSD receiving ravulizumab therapy. This case highlights the complex challenge to prevent NMOSD relapses by maintaining complement inhibition during pregnancy and emphasizes the importance of early diagnosis and management of invasive meningococcal disease.
Methodology
Case presentation
A 32-year-old G4P3 woman at 33+4 weeks’ gestation presented at the emergency department with a 12-hour history of high-grade fever, severe headache, photophobia, neck stiffness, and vomiting. Furthermore, she had suffered progressive confusion for over 2 hours prior to admission. The patient was diagnosed with AQP4-IgG-positive NMOSD in February 2024 following optic neuritis. She was vaccinated against meningococcus prior to initiating therapy, in accordance with recommended guidelines. She received 300 mg ravulizumab intravenously every 8 weeks, with the last dose administered 5 weeks prior to presentation, and she had an uncomplicated pregnancy. On admission, she was critically ill and feverish; her vitals were measured with Temp 39.2°C, her blood pressure was 105/60 mmHg, her heart rate was 118 bpm, and the Glasgow Coma Scale score was 13/15. Neurological examination revealed positive Kernig and Brudzinski signs with no focal neurological deficits.
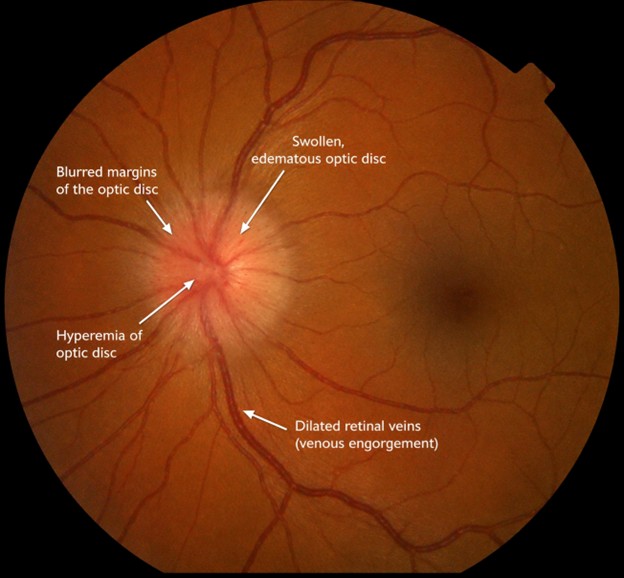
Fundoscopic examination revealed bilateral optic disc swelling with blurred margins, hyperemia, and dilated retinal veins, consistent with Papilledema (Figure 1). These findings were consistent with elevated intracranial pressure, later confirmed by lumbar puncture, which showed increased opening pressure and turbid cerebrospinal fluid.
Moreover, fetal assessment revealed a reactive cardiotocography tracing with no evidence of uterine contractions.
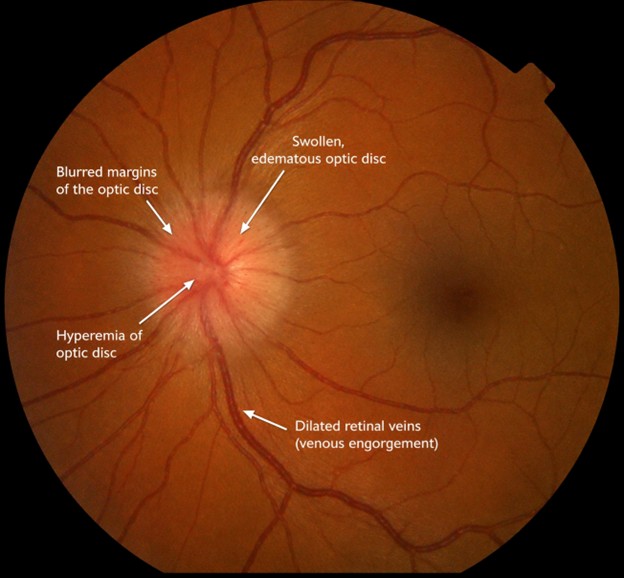
Figure 1: Fundus examination showing bilateral optic disc swelling with blurred margins, hyperemia, and dilated retinal veins, consistent with Papilledema.
Diagnostic Evaluation
White blood cell (WBC) counts were high at 18 × 109/L, C-reactive protein levels were 160 mg/L, and procalcitonin levels were 12 ng/mL. Serum lactate levels were also elevated at 3.2 mmol/L. Lumbar puncture revealed elevated opening pressure and turbid cerebrospinal fluid. Cerebrospinal fluid analysis revealed a leukocyte count of 2500 cells/mm³, a predominance of neutrophils, elevated protein levels, and a decreased glucose concentration. Thus, indicating systemic infection. Gram staining revealed Gram-negative diplococci, and polymerase chain reaction testing further confirmed a Neisseria meningitidis infection. Complement studies demonstrated suppressed CH50 levels, indicating significant inhibition of terminal C5 activity and confirming functional complement blockade at the time of infection. Serum ravulizumab levels were within the therapeutic range. Based on clinical presentation, cerebrospinal fluid findings, and microbiological confirmation, she was diagnosed with acute meningococcal meningitis.
Management
The patient was immediately given intravenous ceftriaxone (2 g twice daily) and intravenous dexamethasone. Given the onset of papilledema, indicated by elevated intracranial pressure, she was transferred to the ICU for close monitoring and supportive care. The fetus was continuously monitored throughout hospitalization.
Owing to complete complement blockade, ravulizumab therapy was temporarily withheld, and serial complement levels were monitored. A multidisciplinary team that involved infectious disease specialists, neurologists, and maternal-fetal medicine physicians managed this rare case of severe infection.
Obstetric Course
On the third day of hospitalization, the patient developed preterm uterine contractions and delivered a male infant vaginally at 34 weeks of gestation. The neonate weighed 2.3 kg and had Apgar scores of 8 at one minute and that of 9 at five minutes. The neonate received empirical intravenous antibiotics as a preventive measure. Subsequently, blood cultures remained negative with no evidence of meningitis.
Neurological Course
Ten days postpartum, the patient developed blurred vision in her right eye. Magnetic resonance imaging demonstrated new optic nerve enhancement, indicating a relapse of NMOSD. After resolution of the meningococcal infection, ravulizumab therapy was reinitiated. The patient also received a short course of intravenous methylprednisolone for relapse management. Thus, she recovered with partial visual improvement. The case timeline is summarized in Figure 2.
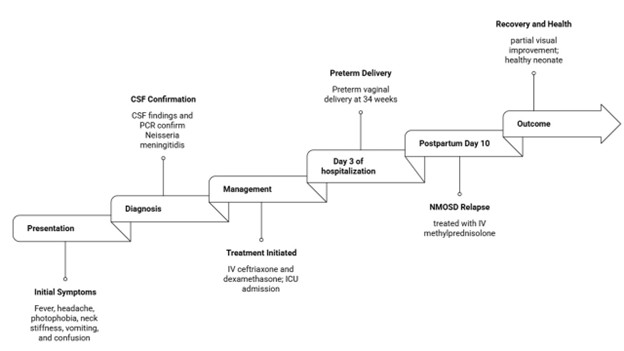
Figure 2: Case Timeline
Discussion
This case describes a rare instance of fulminant meningococcal meningitis in a pregnant patient with AQP4-IgG-positive NMOSD that occurred despite appropriate vaccinations during ravulizumab therapy. It emphasizes the critical challenge of balancing severe infectious risks against NMOSD relapses, particularly when complement inhibitor therapy requires interruption during pregnancy.
Advanced complement therapies have transformed the management of NMOSD. This progress requires a careful trade-off, as blocking this pathway significantly raises a patient's risk for life-threatening meningococcal disease. Compared with other approved complement inhibitors such as eculizumab, inebilizumab, and satralizumab, ravulizumab has a longer half-life and allows dosing intervals of approximately eight weeks while maintaining sustained complement blockade by binding to complement protein C5 and preventing its cleavage into C5a and C5b (9, 10). In the CHAMPION-NMOSD trial, ravulizumab reduced the risk of relapse by 98.6% (11). Nevertheless, inhibition of the terminal complement pathway significantly impairs host defense against encapsulated bacteria, particularly Neisseria meningitidis. For instance, individuals with deficiencies in terminal complement components (C5–C9) have long been recognized as exhibiting markedly increased susceptibility to meningococcal infections (4). Accordingly, an increased risk of meningococcal disease has been reported among individuals receiving complement inhibitor therapy (12). Importantly, breakthrough meningococcal infections have been reported in vaccinated patients receiving complement inhibitors, suggesting that vaccination does not fully eliminate the risk of invasive disease in the setting of terminal complement blockade. Data from surveillance programs in the United States have estimated that the risk of invasive meningococcal disease among patients treated with eculizumab may be up to 1000–2000 times higher than that observed in the general population (7).
In this context, current guidelines strongly recommend vaccination against Neisseria meningitidis before initiation of complement inhibitor therapy, with both quadrivalent conjugate vaccines targeting serogroups A, C, W, and Y, and vaccines directed against serogroup B (13). However, vaccination does not eliminate the risk of infection. Breakthrough infections have been reported despite appropriate immunization, particularly in individuals treated with eculizumab or related agents. This reduced protection is attributed to persistent blockade of membrane attack complex–mediated bacterial lysis, as well as the emergence of less common or atypical N. meningitidis strains that may cause invasive disease in the setting of impaired complement function (14).
Papilledema observed in this case was attributed to increased intracranial pressure secondary to acute meningitis caused by Neisseria meningitidis. Elevated cerebrospinal fluid pressure is transmitted to the optic nerve sheath, resulting in impaired axoplasmic flow and optic disc edema. Similar findings have been reported in severe central nervous system infections associated with raised intracranial pressure (15). In contrast, optic neuritis associated with NMOSD represents inflammatory demyelination of the optic nerve. It typically presents with acute visual impairment, pain with eye movement, and optic nerve enhancement on magnetic resonance imaging rather than isolated pressure-related disc swelling. Previous neuro-ophthalmologic studies and NMOSD case reports have emphasized the importance of differentiating papilledema from inflammatory optic neuritis using clinical presentation, cerebrospinal fluid pressure findings, fundoscopic appearance, and neuroimaging (16-19).
Pregnancy is associated with immunological changes that may influence the course of neuromyelitis optica spectrum disorder, with several studies suggesting an increased risk of relapse in the postpartum period (20, 21). Additionally, therapeutic monoclonal antibodies such as ravulizumab share structural similarities with endogenous IgG and are therefore capable of crossing the placental barrier (8). Recent study by Jacob et al. (22) reported the transplacental transfer of ravulizumab in a case of a pregnant woman with NOMSD. In the present case, the neonate remained clinically stable and showed no evidence of meningococcal infection. Nevertheless, the potential effects of maternal complement inhibitor therapy on neonatal immunity remain an area requiring further investigation. Monitoring neonates born to mothers receiving complement inhibitors may be recommended, particularly when exposure occurs during the third trimester.
Table 1 summarizes prior study results of pregnancy cases involving complement inhibitor therapy and associated maternal and neonatal outcomes.
|
Table 1: Summary of reported pregnancy and complement inhibitor–related outcomes in NMOSD and related conditions |
|||||
|
Author |
Condition |
Therapy |
Pregnancy/Neonatal Outcome |
Infection |
Key Finding |
|
Jacob et al., 2025 (22) |
NMOSD |
Ravulizumab |
Healthy neonate; no complications |
No |
First evidence of transplacental ravulizumab transfer |
|
Seyed Ahadi et al., 2021 (21) |
NMOSD |
Rituximab |
50% live births; no major malformations; 1 IUFD; 2 medically terminated pregnancies |
No serious infections |
Maternal rituximab exposure showed generally favorable pregnancy outcomes |
|
Guerra et al., 2025 |
NMOSD |
Eculizumab |
Live birth of healthy infant |
No |
Successful pregnancy continuation under complement inhibition |
|
Füreder et al., 2025 (24) |
PNH |
Ravulizumab |
Uneventful pregnancy; normal fetal development |
No |
Suggests early pregnancy safety of ravulizumab |
|
McNamara et al., 2017 (7) |
PNH |
Eculizumab |
Not pregnancy-specific outcome |
16 cases meningococcal disease; 1 death |
High risk of breakthrough meningococcal infection despite vaccination |
|
Present case |
NMOSD |
Ravulizumab |
Preterm delivery; neonatal stable; postpartum relapse |
Fulminant meningococcal meningitis |
First reported severe infection with postpartum relapse during therapy interruption |
|
PNH: paroxysmal nocturnal hemoglobinuria; NMOSD: Neuromyelitis optica spectrum disorder |
|||||
Another challenge is the therapeutic dilemma posed by interrupting complement inhibitor therapy during severe infection. Discontinuation of ravulizumab was necessary to allow recovery of complement activity and treat the ongoing bacterial infection. However, complement inhibition is the primary mechanism through which ravulizumab prevents NMOSD relapse. The temporal association between cessation of ravulizumab therapy and subsequent postpartum optic neuritis raises the possibility of NMOSD relapse during a high-risk period. Similar rebound disease activity has been reported in patients with NMOSD following interruption of immunosuppressive therapy (23).
Management of NMOSD during pregnancy requires special clinical considerations; cases require careful coordination between neurology, infectious disease, and maternal-fetal medicine specialists. Prompt antimicrobial therapy remains the cornerstone of treatment for meningococcal infections. In addition, early recognition of neurological relapses is essential to allow rapid reinitiation of disease-modifying therapy once infection has resolved. Short courses of high-dose corticosteroids remain a standard treatment for acute NMOSD relapses and were used successfully in this case.
Clinical Implications
This case report provides detailed clinical, laboratory, and therapeutic information, including monitoring of complement activity at the time of infection. Additionally, it underscores the dilemma caused by the interruption of complement inhibitor therapy, which carries a risk of NMOSD relapse, particularly during the postpartum period when disease activity may increase due to immunomodulatory effects. However, further research is needed to better define optimal strategies for infection prevention in patients receiving complement inhibitors. In addition, prospective longitudinal studies examining pregnancy outcomes in women receiving complement inhibitors would provide valuable information for clinical decision-making.
Strengths and Limitations
This case report is limited by the inability to generalize the findings and by limited investigations into the potential effects of maternal complement inhibitor therapy on neonatal immunity. However, it has an educational value, providing more understanding of a rare, poorly understood condition, the comprehensive clinical history obtained, and the adequate diagnostic investigations performed.
Conclusion
Being a recurring autoimmune disease with life-threatening complications, the management of NMOSD is challenging, particularly during pregnancy. This is attributed to immunomodulatory changes, with higher relapse rates reported prepartum and postpartum. Despite the efficacy of ravulizumab and other complement inhibitors used in treatment, they increase the risk of infections, particularly from Neisseria meningitidis. This rare case demonstrates the therapeutic dilemma in managing NMOSD during pregnancy, where continuing treatment carries the risk of infection and stopping the drug could potentially lead to a relapse. Further studies and longitudinal monitoring of exposed infants are essential to establish safety and clinical guidelines.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Ethical consideration
Written informed consent was obtained from the patient for the publication of this case report.
Data availability
All data is available within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.