Volume 6, Issue 5
May 2026
When Venom Meets the Coronary Artery: Anterior STEMI Following Exposure to Snake Envenomation: A Case Report
Ahmed A. Alhazmi, Abdullah S. Alrajhi, Abdullatif H. Ujaimi, Wajd Y. Asssahafi, Omar S. Almogheer
DOI: http://dx.doi.org/10.52533/JOHS.2026.60501
Keywords: Myocardial infarction, Snake envenomation, ST-segment elevation myocardial infarction, Acute coronary syndrome
Background: Snake envenomation is a globally recognized neglected tropical disease that remains uncommon but potentially a catastrophic cause of cardiovascular toxicity. It has been documented to have hemotoxic and neurotoxic effects, along with its ability to induce direct myocardial ischemia, malignant arrhythmias, and cardiogenic shock that is often underestimated, particularly in non-endemic regions. Venom components can trigger a "thrombotic storm" through direct endothelial injury and hypercoagulability, posing significant diagnostic and therapeutic challenges for cardiology teams.
Case presentation: Our case describes a 72-year-old Moroccan man with no documented prior comorbidities who presented to the emergency department with a one-week history of progressive dyspnea, orthopnea, and palpitations, later confirmed to have an acute anterior ST-segment elevation myocardial infarction (STEMI). He was immediately referred to our center for lifesaving intervention. Coronary angiography revealed a total proximal left anterior descending (LAD) artery occlusion in the absence of diffuse atherosclerotic disease. Despite successful primary percutaneous coronary intervention (PCI) with restoration of Thrombolysis in Myocardial Infarction (TIMI) grade III flow, the patient developed recurrent ventricular tachycardia and refractory cardiogenic shock. A subsequent physical examination revealed a bleeding wound on the right shoulder with two distinct pinpoint puncture marks, raising a high clinical suspicion of snake envenomation. Despite aggressive resuscitation efforts and a consultation with the National Toxicology Center for antivenom administration, the patient suffered a final pulseless cardiac arrest and was pronounced dead.
Conclusion: This case highlights a rare but lethal intersection between snake envenomation and the development of acute myocardial infarction. It highlights a paradox where dual antiplatelet therapy might be neutralized by venom-derived enzymes, leading to rapid clinical deterioration despite successful mechanical revascularization. These findings emphasize that envenomation must remain part of the differential diagnosis in cases of atypical STEMI. Early clinical recognition, multidisciplinary collaboration with toxicology experts, and the availability of anti-venom therapy even in regions where snake bites are uncommon are critical factors for improving survival.
Introduction
The World Health Organization (WHO) has recognized snake envenomation as a neglected tropical disease. It poses a significant global health burden and accounts for substantial morbidity and mortality. The impact is underestimated due to limited data (1, 2).
Cardiovascular manifestations are uncommon but potentially fatal. They range from hypotension to malignant ventricular arrhythmias, cardiac arrest, and death (3). Despite their major consequences, these manifestations remain poorly understood. They are thought to be mediated by multiple venom-related mechanisms. Venom components such as phospholipases A2 and bradykinin-potentiating peptides affect the heart muscle, vascular smooth muscles, and the capillary bed (3,4).
Acute coronary syndromes, particularly ST-segment elevation myocardial infarction (STEMI), are most commonly caused by atherosclerotic plaque rupture with superimposed thrombosis (6). However, myocardial ischemia following snake envenomation has been reported to occur through coronary vasospasm, endothelial injury, systemic shock, or a prothrombotic state, even in the absence of pre-existing coronary artery disease (7-9).
We report a rare case of anterior STEMI complicated by refractory ventricular arrhythmia and cardiogenic shock in the context of suspected snake envenomation, underscoring the importance of interdisciplinary collaboration and awareness in non-endemic regions.
Case presentation
A 72-year-old Moroccan male without a clear medical history was referred to our facility via the cardiac hotline as a lifesaving case of acute anterior STEMI with evidence of pulmonary edema.
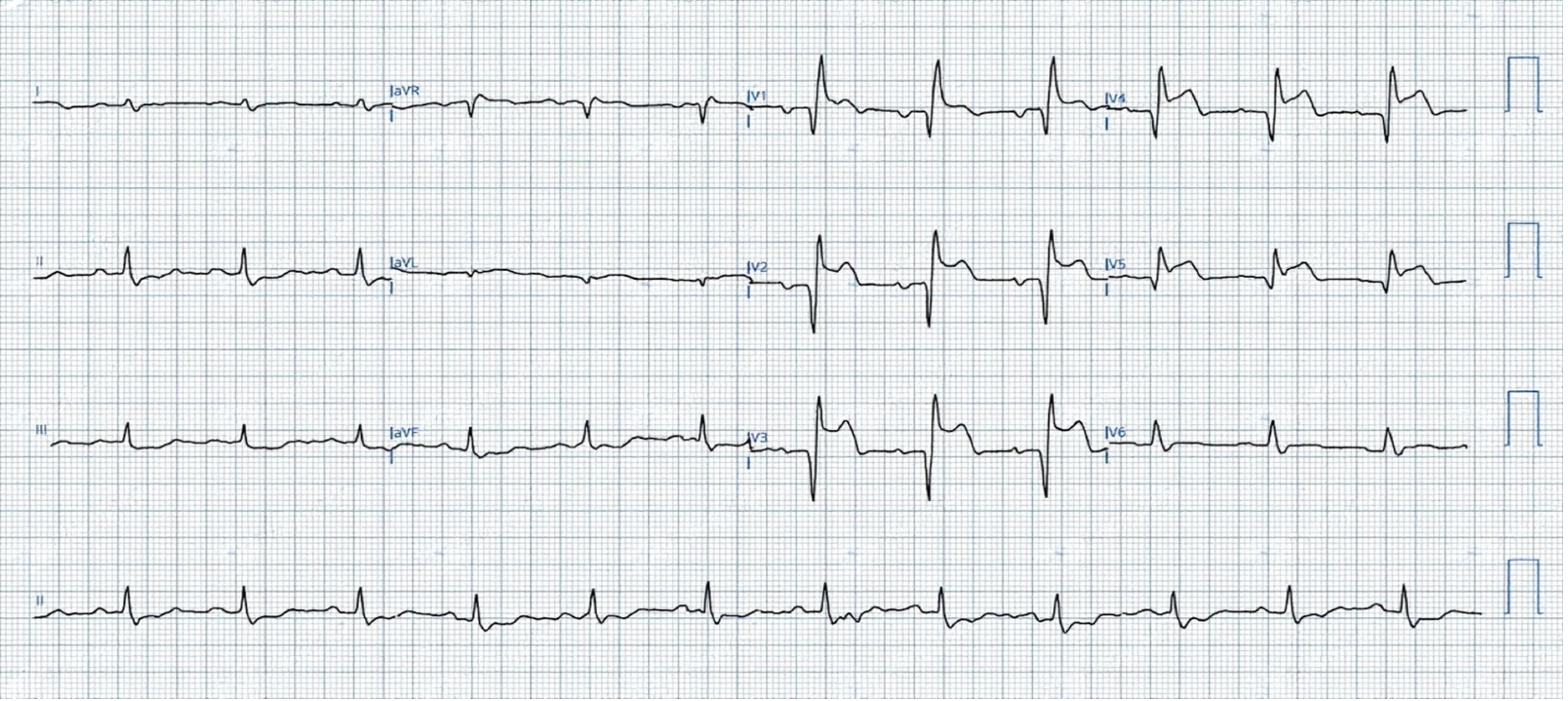
The patient presented with a one-week history of progressive shortness of breath associated with orthopnea and palpitations. Upon arrival at the referring emergency department, he was tachycardic and hypoxic, with a pulse rate of 120 bpm, blood pressure of 121/72 mmHg, oxygen saturation of 90% on room air, and he was afebrile at 37 C. An electrocardiogram (ECG) revealed an acute anterior STEMI (Figure 1) for which he received loading doses of aspirin, clopidogrel, and a heparin bolus before urgent transfer for coronary intervention.
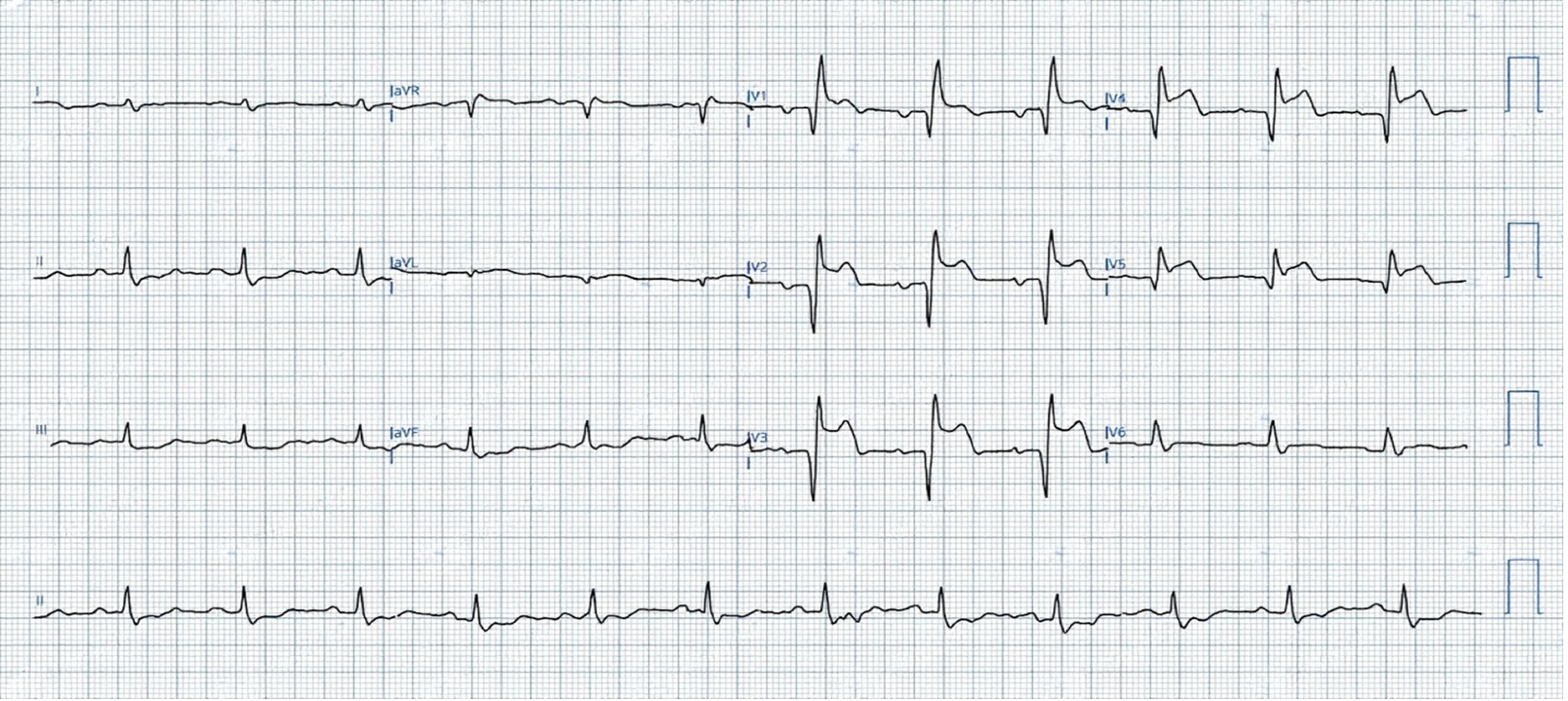
Figure 1: an electrocardiogram showing ST elevation in V1-V5, ST depression in leads II, III, and aVF.
Upon arrival at our cardiac day care unit, the patient was conscious and oriented but appeared distressed and hemodynamically unstable with a pulse rate of 120 bpm, Blood pressure of 115/59 mmHg, and an oxygen saturation of 96% on room air. Blood samples were obtained, and the patient was immediately transferred to the catheterization laboratory. A coronary angiogram performed through a right radial approach revealed total thrombotic occlusion of the proximal segment of the left anterior descending artery (LAD) and a co-dominant right coronary artery (RCA) with a tight proximal lesion without other significant disease (Figure 2A).
During the procedure, the patient developed a wide-complex tachyarrhythmia (HR 220 bpm) and became unstable, requiring multiple synchronized cardioversions and subsequent intubation.
Primary percutaneous coronary intervention (PCI) to the LAD was performed with balloon dilatation and stenting using one drug-eluting stent (3.0 x 30 mm). TIMI III flow was successfully restored (Figure 2B), and the patient was transferred to the cardiac care unit (CCU).
A bedside echocardiography study showed severely reduced left ventricular systolic function with an ejection fraction (EF) of 10%, global hypokinesia, mild mitral, aortic, and tricuspid regurgitation. A portable chest x-ray demonstrated bilateral pulmonary congestion with obliterated costophrenic angles (Figure 3). Initial laboratory workup results are summarized (Table 1).
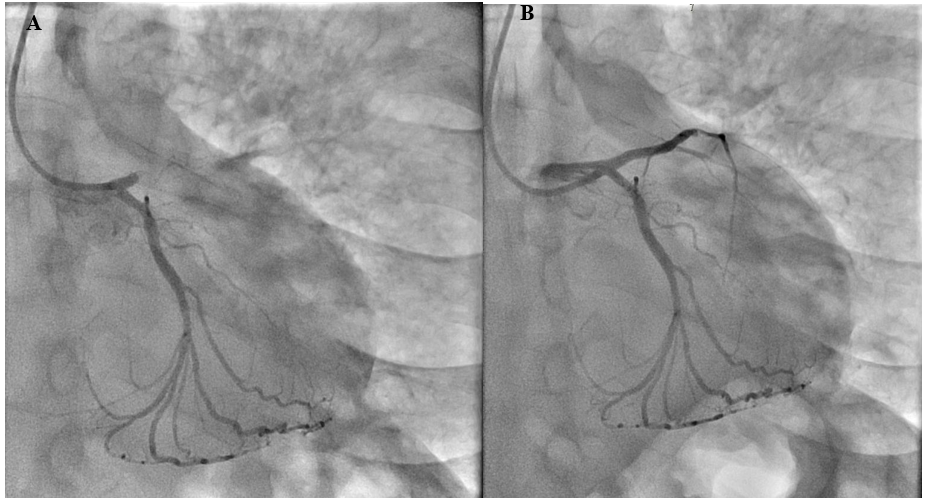
Figure 2: A) filling defect in the proximal left anterior descending artery with reduced contrast flow. B) Post-primary percutaneous coronary intervention showing TIMI III flow.
Figure 3: Portable chest x-ray anterior-posterior view showing bilateral congested lungs.
|
Table 1: Summary of laboratory findings at presentation |
||
|
Patient’s results |
Laboratory reference range |
|
|
Hemoglobin (g/L) |
116 |
115 - 165 |
|
Mean corpuscular volume (flu) |
89.0 |
80 - 101 |
|
Mean corpuscular hemoglobin (pg) |
30.0 |
27 - 34 |
|
Leukocytes: WBC count (109/ul) |
18.9 |
4 - 11 |
|
Platelet count (109/ul) |
511 |
140 - 450 |
|
Creatinine (µmol/L) |
122 |
44 - 90 |
|
Blood urea nitrogen (mmol/L) |
19.8 |
2.7 – 8.2 |
|
Sodium (mmol/L) |
122 |
135 - 145 |
|
Chloride (mmol/L) |
89 |
98-107 |
|
Phosphorus (mmol/L) |
1.92 |
0.78-1.65 |
|
Potassium (mmol/L) |
4.4 |
3.5 – 5.1 |
|
Alanine transaminase (U/L) |
189 |
10 - 34 |
|
Aspartate transaminase (U/L) |
287 |
10 - 34 |
|
Prothrombin time (sec) |
21.5 |
9.8 – 15.3 |
|
International normalized ratio (INR) |
1.75 |
0.8 – 1.2 |
|
Partial thromboplastin time (sec) |
120 |
26 – 40 |
In the CCU, the patient experienced recurrent ventricular tachycardia (VT) treated with amiodarone, magnesium sulfate, lidocaine, and sodium bicarbonate. He remained hemodynamically unstable, necessitating further cardioversion and norepinephrine infusion. Dual antiplatelet therapy (DAPT) with aspirin and ticagrelor was commenced alongside tirofiban. Physical examination revealed a bleeding right shoulder wound that raised suspicion of a snake bite due to the presence of two distinct pinpoint puncture marks surrounded by erythema (Figure 4). The National Toxicology Center recommended administration of a polyvalent snake antivenom and tetanus prophylaxis, which was unavailable at the time. However, before the antivenom could be administered, the patient developed recurrent pulseless VT. Despite prolonged cardiopulmonary re resuscitation, return of spontaneous circulation was not achieved. The patient was pronounced dead and transferred for postmortem care.

Figure 4: A wound with two tiny puncture marks surrounded by erythema and active beeding.
Discussion
This case illustrates a diagnostically complex scenario of acute anterior STEMI complicated by malignant arrhythmia and cardiogenic shock following a suspected snakebite in an elderly male patient without other comorbidities. Although snakebites are prevalent in Saudi Arabia, where a high local prevalence of venomous species has been reported, the number of published studies on victims remains infrequent, outdated, and fragmented (1).
While a recent large Saudi cohort study reported systemic complications such as neurotoxicity, coagulopathy, and acute kidney injury, no cases of STEMI were identified (10). Currently, there are no published reports of STEMI caused by snakebites in Saudi Arabia, and globally, the literature remains sparse. This highlights the exceptional nature of this case.
In most clinical settings, STEMI is caused by atherosclerotic plaque rupture, and the standard of care is rapid revascularization (6). However, as reported by Niraj et al. and Roplekar et al., snake envenomation can precipitate myocardial infarction through alternative, less-understood mechanisms, including direct endothelial injury, coronary vasospasm, and a systemic prothrombotic state, theoretically altering the management plan (8, 9).
Unlike most reported cases by Ramakrishna and Placid, Lucia et al, and Saadeh, where angiography revealed normal coronaries post-envenomation (5, 11, 12), our patient, similar to a case reported by Simpson et al, presented with a thrombus-induced occlusion in the absence of significant underlying atherosclerosis (13). In that instance, the patient achieved a full recovery following the administration of 14 vials of anti-venom alongside PCI.
The rapid deterioration and eventual death despite successful mechanical revascularization in our patient raise the suspicion of profound myocardial electrical instability and underscore the potential significance of antivenom to act as a definitive treatment in such cases.
Beyond venom-induced vasospasm, venom-derived ADPases and fibrinogenolytic proteins may have interfered with platelet inhibition, potentially reducing the efficacy of DAPT (14). While the Simpson case suggests that standard antiplatelet and anticoagulation therapies can be tolerated in some envenomations, our patients' rapid decline, as summarized (Figure 5), supports the theory that in the absence of neutralizing antivenom, the enzymatic activity of the venom may continue to promote microvascular damage and a hypercoagulability state that exceeds the capabilities of DAPT.
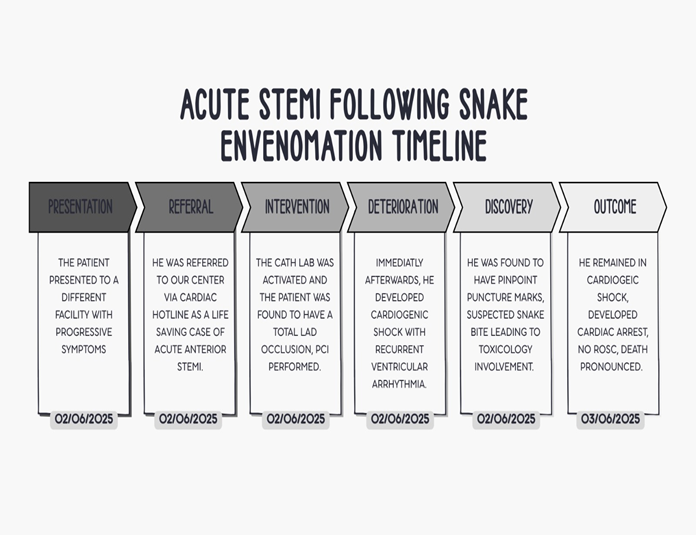
Figure 5: A timeline of the patient’s presentation and hospital course.
Furthermore, the coexistence of myocardial ischemia, malignant arrhythmias, and systemic venom toxicity likely produced a synergistic cascade leading to irreversible cardiogenic shock and death.
This case sheds light on critical challenges that include delayed recognition of envenomation, limited antivenom availability, and complex drug interactions. Early involvement of toxicology experts and timely anti-venom administration may improve outcomes.
This case sheds light on critical challenges that include delayed recognition of envenomation, limited antivenom availability, and complex drug interactions. Early involvement of toxicology experts and timely anti-venom administration may improve outcomes.
Conclusion
Snake envenomation is a rare but critical differential diagnosis in acute STEMI, even in non-endemic regions. Venom components can precipitate coronary occlusion, arrhythmia, and cardiogenic shock. Prompt recognition, early toxicology intervention, and access to antivenom are crucial for improving survival.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Ethical consideration
None.
Data availability
All data is available within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.