Volume 6, Issue 3
March 2026
Awareness of Selective Serotonin Reuptake Inhibitors’ Discontinuation Symptoms Among Physicians and Residents in Psychiatry and Family Medicine in Riyadh City
Lujain Mohammed Althagafi, Naif Y. Alfrayyan, Aqeel A. Almarhoon, Mohammed Saud Almubaddil, Reema Abdulaziz Alageel, Fatimah Abdullah Alrashed, Atha Abdulrhman Alghazi, Abeer Abdulrahman Alangari, Taif Madhi Alboqami, Latifah Abdulrahman Albehairi
DOI: http://dx.doi.org/10.52533/JOHS.2026.60303
Keywords: Selective Serotonin Reuptake Inhibitors (SSRIs), Antidepressant Discontinuation Syndrome, Physician Awareness, Withdrawal Symptoms, Primary Health Care, Saudi Arabia
Background: Antidepressant Discontinuation Syndrome (ADS) frequently mimics depressive relapse, rebound in anxiety, or somatic symptoms that make the patient worry more, creating significant diagnostic challenges in clinical practice. Despite the high prescription rates of Selective Serotonin Reuptake Inhibitors (SSRIs), data regarding physician awareness of ADS in Saudi Arabia remain scarce. This study assessed the awareness, clinical observations, and educational needs regarding ADS among psychiatrists and family physicians in Riyadh.
Methodology: A cross-sectional study was conducted in Riyadh, Saudi Arabia, from January 2025 to November 2025. The study population included 129 physicians (consultants, specialists, and residents) specializing in Psychiatry and Family Medicine. Data were collected using a validated online self-administered questionnaire derived from the Discontinuation-Emergent Signs and Symptoms (DESS) checklist. Statistical analysis was performed using SPSS version 26, with significance set at p < 0.05.
Results: Of the 129 physicians. 57.4% reported encountering patients with ADS. A significant gap in active recall was evident; only 23.9% spontaneously recalled anxiety, compared to 89.4% who recognized it when prompted. Psychiatrists were significantly more likely to report clinical encounters with ADS (75.7%) compared to family physicians (24.3%). Additionally, junior clinicians identified the symptom of insomnia more so than seniors (p=0.003), and 30% of respondents reported inconsistent patient education regarding withdrawal effects.
Conclusion: ADS is a prevalent clinical reality in Riyadh, yet physician awareness remains fragmented, particularly within primary care settings. The disparity between passive recognition and active recall highlights a critical vulnerability, necessitating targeted Continuing Medical Education (CME) to ensure safe patient management.
Introduction
Selective Serotonin Reuptake Inhibitors (SSRIs) have revolutionized the pharmacological management of psychiatric conditions since their introduction in the late 1980s. Currently, they serve as the gold-standard, first-line treatment for major depressive disorder (MDD), generalized anxiety disorder (GAD), panic disorder, and obsessive-compulsive disorder (OCD) due to their efficacy and comparatively favourable safety profiles when weighed against older tricyclic antidepressants (TCAs) or monoamine oxidase inhibitors (MAOIs) (1, 2). As global mental health awareness increases, the prescription rates for SSRIs have surged exponentially. Recent data indicate that antidepressant consumption has nearly doubled in many developed nations over the last two decades, solidifying their place as some of the most frequently prescribed medications in modern medicine (3, 4).
The sudden cessation or rapid tapering of the SSRIs can trigger Antidepressant Discontinuation Syndrome (ADS), a complex withdrawal phenomenon characterized by physiological dependence. ADS is hypothesized to be a state of transient serotonin hypofunction. Because SSRIs maintain high levels of synaptic serotonin, the brain’s post-synaptic receptors undergo down-regulation to maintain homeostasis. When the drug is abruptly removed, the brain is left with a deficit of available serotonin and a diminished receptor sensitivity, leading to a systemic "rebound" effect (5, 6). The condition is characterized by somatic, neurological, and affective symptoms; patients frequently report debilitating headaches, dizziness, paraesthesia (often described as "brain zaps"), flu-like lethargy, and acute spikes in anxiety (7, 8). While many clinical guidelines historically characterized ADS as a mild, self-limiting condition lasting only one to two weeks, emerging patient-led data and longitudinal studies suggest a more arduous reality. Symptoms can persist for months, and while the general incidence is estimated at 15%, approximately 3% of patients experience severe, life-altering withdrawal (9, 10, 11). Specific risk factors, such as longer treatment duration and shorter drug half-life, significantly increase the probability of severe withdrawal symptoms (12).
One of the most clinical challenges is distinguishing ADS from relapse of the underlying psychiatric disorder, such as irritability or insomnia, which frequently leads clinicians to misinterpret ADS as a depressive relapse or a "rebound" of the underlying anxiety disorder. The symptomatic overlap often leads to misdiagnosis, which carries heavy consequences: it often results in the unnecessary resumption of medication, the initiation of higher doses, or the introduction of additional psychotropic drugs, thereby the patient enters a cycle of polypharmacy (13, 14). Beyond the physiological toll, mismanaged discontinuation can severely erode the therapeutic alliance, leaving patients feeling unheard and fearful of future pharmacotherapy (13).
Therefore, physicians’ awareness regarding tapering protocols and symptom recognition is critical. Gaps exist in clinician knowledge regarding this syndrome; many general practitioners do not consider their knowledge of withdrawal effects adequate or feel confident in distinguishing withdrawal symptoms from relapse (15).
Currently, there are no data regarding the awareness of ADS among physicians in Saudi Arabia. This knowledge gap is particularly pressing. As the Kingdom undergoes a massive healthcare transformation under Vision 2030, there is an increasing emphasis on decentralizing mental healthcare and integrating these services into primary care settings (16). This study assesses the level of awareness, clinical observations, and educational needs regarding SSRIs discontinuation among psychiatrists, family physicians, and residents in these specialties in Riyadh, Saudi Arabia.
Methodology
Study Design and Setting
This cross-sectional questionnaire-based study was carried out in Riyadh, Saudi Arabia. The study period extended from January 2025 through November 2025.
Participants and Sampling
The study subjects included psychiatrists, and Family Medicine physicians, and residents living in Riyadh, Saudi Arabia. Participants were recruited using convenience sampling.
The study included physicians of all ranks (Residents, Specialists, and Consultants) practicing Psychiatry or Family Medicine within both government and private sectors in Riyadh City. Interns, medical students, physicians from other specialties, and those physicians from other specialties, and those practicing outside Riyadh were excluded.
Sample Size
The minimum sample size was calculated to be 128 participants. This calculation was based on an expected awareness prevalence of 70% with a ±10% margin of error, a statistical power of 80%, and a 95% confidence level.
Data Collection and Instrument
Data was collected using a survey link via "Google Forms." The survey was distributed through Email, WhatsApp, Twitter or X, and Telegram. The platform was configured to allow one answer per email address to avoid duplication. Participants were asked to complete surveys individually. The questionnaire was designed to fulfil the study objectives, including assessing the level of awareness among physicians about discontinuation symptoms of SSRIs, determining their prevalence, and identifying the most common symptoms observed.
Validity
The specific list of potential symptoms provided in the survey was derived from the validated Discontinuation-Emergent Signs and Symptoms (DESS) checklist and established clinical trials (17, 18) to ensure comprehensive coverage of somatic and psychological manifestations.
Statistical Analysis
The statistical analysis was conducted using IBM SPSS (Statistical Package for the Social Sciences) software, version 26. Descriptive statistics were used to present the data. Categorical variables were reported as frequencies and valid percentages. The Association between categorical variables was examined using the Chi-Square test. Statistical significance was considered when the P value was less than 0.05.
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) at King Abdullah Bin Abdulaziz University Hospital (Log Number: 25-0002) on January 28, 2025.
Results
Our study involved 129 surveyed physicians and Residents in Psychiatry and Family Medicine in Riyadh City. The majority were family medicine physicians (n=66, 51.2%), followed by psychiatry physicians (n=63, 48.8%). Many physicians (n=113, 87.6%) reported familiarity with discontinuation symptoms associated with selective serotonin reuptake inhibitors (SSRIs), most of them acquired with residency or fellowship training and personal clinical experience (71.7%), followed by medical literature or research (23.0%), and other methods such as Continuing Medical Education (CME) programs, workshops, or social media (5.3%). Among 113 familiar physicians, years of post-graduation clinical practice were distributed across 0–2 years (37.2%), 3–5 years (32.7%), and six or more years (30.1%), with the majority working in public sector hospitals (95.6%) compared to private sector ones (4.4%), as indicated in Table 1.
|
Table 1: Demographic characteristics for the Physicians in Riyadh City (N=129) |
|||
|
Factor |
Category |
Number |
Percent |
|
What is your specialty? |
Family Medicine |
66 |
51.2 |
|
Psychiatry |
63 |
48.8 |
|
|
Are you familiar with the discontinuation symptoms associated with Selective Serotonin Reuptake Inhibitors? |
No |
16 |
12.4 |
|
Yes |
113 |
87.6 |
|
|
If yes, how did you acquire this knowledge? (N=113) |
Medical literature/research |
26 |
23.0 |
|
Residency or fellowship training / personal clinical experience |
81 |
71.7 |
|
|
Other* |
6 |
5.3 |
|
|
Years of clinical practice after graduation (N=113) |
0–2 years |
42 |
37.2 |
|
3–5 years |
37 |
32.7 |
|
|
6 years or more |
34 |
30.1 |
|
|
Current workplace (N=113) |
Private Sector Hospitals |
5 |
4.4 |
|
Public Sector Hospitals |
108 |
95.6 |
|
|
Other*: CME programs/workshops, social media |
|||
Out of the 129, 113 physicians are familiar with SSRI discontinuation symptoms, when asked to list three from memory, the most commonly reported were headache (38.1%), insomnia (31.0%), flu-like symptoms (26.5%), and anxiety (23.9%), with all respondents mentioning many other symptoms" such as limb numbness, irritability, panic, and palpitations. When the physicians selecting known associated symptoms, a strong majority recognized anxiety, agitation, panic, depression, irritability, aggression, anger, and bouts of crying (89.4%); insomnia, nightmares, hypersomnia, and lethargy (77.0%); balance problems and dizziness (72.6%); and other symptoms (95.6%) including decreased concentration, amnesia, gastrointestinal issues, intensification of suicidal ideation, sweating, flushing, chills, tremor, myoclonus, muscle aches, facial numbness, visual symptoms, paraesthesia, tinnitus, myalgias, and premature ejaculation (Table 2).
More than half (57.4%) reported having seen patients who experienced these symptoms after stopping SSRIs abruptly, with the most frequently noted issues being related to anxiety (71.6%), flu-like symptoms, fatigue, weakness, and tiredness (70.3%), sleep disturbances, including insomnia (58.1%), balance issues and dizziness (48.6%), and a large range of other symptoms (81.1%).
Regarding patient education, physicians indicated that they always (38.1%), often (31.9%), sometimes (22.1%), rarely (4.4%), or never (3.5%) informed patients and caregivers about possible withdrawal symptoms. To enhance awareness of SSRI discontinuation symptoms, respondents favoured continuing medical education programs (36.3%), other measures such as social media, workshops, and seminars (24.8%), lectures (21.2%), and collaboration between specialties (17.7%), as indicated in Table 2.
|
Table 2: Physicians’ Knowledge and Awareness Regarding SSRI Discontinuation Symptoms (N=113) |
|||
|
Factor |
Category |
Number |
Percent |
|
From your memory, list three symptoms of discontinuation of SSRIs |
|||
|
Headache |
No |
70 |
61.9 |
|
Yes |
43 |
38.1 |
|
|
Insomnia |
No |
78 |
69.0 |
|
Yes |
35 |
31.0 |
|
|
Flu-like symptoms |
No |
83 |
73.5 |
|
Yes |
30 |
26.5 |
|
|
Anxiety |
No |
86 |
76.1 |
|
Yes |
27 |
23.9 |
|
|
Other* |
Yes |
113 |
100 |
|
Select the symptoms you know are associated with SSRI discontinuation |
|||
|
Anxiety, agitation, panic, depression, irritability, aggression, anger, and bouts of crying |
No |
12 |
10.6 |
|
Yes |
101 |
89.4 |
|
|
Balance problems, dizziness |
No |
31 |
27.4 |
|
Yes |
82 |
72.6 |
|
|
Insomnia, nightmares, hypersomnia, lethargy |
No |
26 |
23.0 |
|
Yes |
87 |
77.0 |
|
|
Other ** |
No |
5 |
4.4 |
|
Yes |
108 |
95.6 |
|
|
Have you encountered patients who have experienced discontinuation symptoms after abruptly stopping SSRIs? |
No |
39 |
30.2 |
|
Yes |
74 |
57.4 |
|
|
If yes, please describe your experience and the most common symptoms observed (N=74) |
|||
|
Flu-like symptoms, fatigue, weakness, tiredness |
No |
22 |
29.7 |
|
Yes |
52 |
70.3 |
|
|
Insomnia, nightmares, hypersomnia, lethargy |
No |
31 |
41.9 |
|
Yes |
43 |
58.1 |
|
|
Balance problems, dizziness |
No |
38 |
51.4 |
|
Yes |
36 |
48.6 |
|
|
Anxiety, agitation, tension, panic, depression, intensification of suicidal ideation, irritability, impulsiveness, aggression, anger, and bouts of crying |
No |
21 |
28.4 |
|
Yes |
53 |
71.6 |
|
|
Other** |
No |
14 |
18.9 |
|
Yes |
60 |
81.1 |
|
|
How often do you inform patients and caregivers of the possible withdrawal symptoms on cessation of antidepressant treatment? (N=113) |
Always |
43 |
38.1 |
|
Often |
36 |
31.9 |
|
|
Sometimes |
25 |
22.1 |
|
|
Rarely |
5 |
4.4 |
|
|
Never |
4 |
3.5 |
|
|
In your opinion, which of the following measures can be taken to enhance awareness and knowledge about discontinuation symptoms? (N=113) |
Collaboration between different Specialties |
20 |
17.7 |
|
Continuing Medical Education (CME) Programs |
41 |
36.3 |
|
|
Lectures |
24 |
21.2 |
|
|
Other*** |
28 |
24.8 |
|
|
Other*: limb numbness, irritability, panic, Palpitations, difficulty sleeping, depression, mood swings, electrical sensations, suicidal thoughts, low mood, Drowsiness, Dizziness, GI distress, diarrhea, paresthesia. Other**: Decreased concentration, amnesia, Gastrointestinal symptoms (nausea, vomiting, diarrhea, anorexia, abdominal pain), Intensification of suicidal ideation, sweating, flushing, chills, Tremor, myoclonus, muscle aches, facial numbness, Visual symptoms (visual changes, blurred vision), Paresthesia, tinnitus, myalgias, Premature ejaculation. Other***: social media, Workshops, and Seminars |
|||
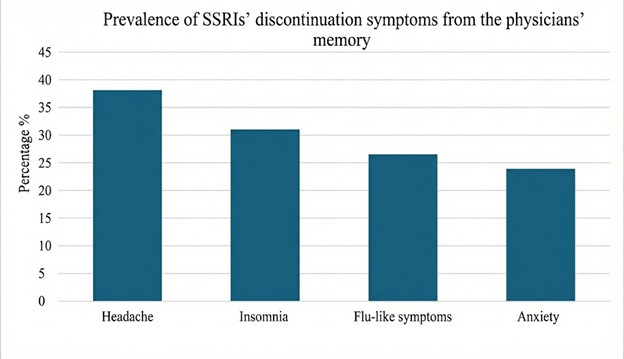
Figure 1 illustrates the prevalence of SSRIs’ discontinuation symptoms from physicians’ memories among 113 physicians. Most physicians reported Headache (38.1%), Insomnia (31.0%), Flu-like symptoms (26.5%), and Anxiety (23.9%).
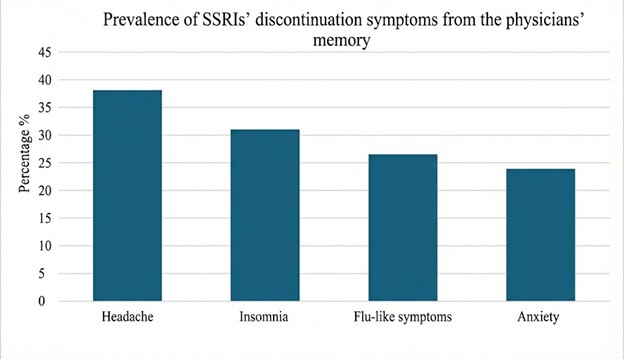
Figure 1:Prevalence of SSRIs’ discontinuation symptoms from the physicians’ memory
Figure 2 illustrates the Discontinuation symptoms of SSRIs observed by the physicians. Out of the 74 physicians encountered, patients who have experienced discontinuation symptoms after abruptly stopping SSRIs, Anxiety, agitation, tension, panic, depression, intensification of suicidal ideation, irritability, impulsiveness, aggression, anger, and bouts of crying were the most observed symptoms among the physicians (71.6%), Flu-like symptoms, fatigue, weakness, tiredness (70.3%), followed by Insomnia, nightmares, hypersomnia, lethargy (58.1%) and then Balance problems, dizziness (48.6%).
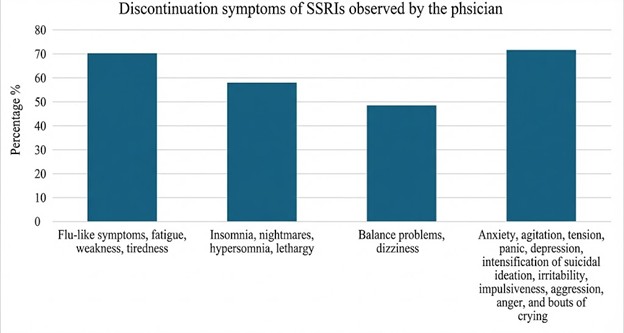
Figure 2:The most common observed symptoms by physicians
Table 3 summarizes the relationship between physicians' familiarity with SSRIs’ discontinuation symptoms and their specialties. A significant difference (p=0.010) was observed in the specialty of the physician: psychiatry physicians had greater familiarity with SSRIs’ discontinuation symptoms than family medicine physicians (n=60, 95.2%).
|
Table 3: Association between Familiarity of the physician with the SSRIs’ discontinuation symptoms and their specialties |
||||
|
Factor |
Category |
Familiarity with the SSRIs’ discontinuation symptoms N (%) |
P-Value |
|
|
No |
Yes |
|||
|
What is your specialty? |
Family Medicine |
13 (19.7) |
53 (80.3) |
0.010* |
|
Psychiatry |
3 (4.8) |
60 (95.2) |
||
|
*Chi-square test |
||||
Figure 3 illustrates the methods suggested by the physicians to improve Awareness and Knowledge of SSRI Discontinuation Effects. Most of the 113 physicians (36.3%) suggested Continuing Medical Education Programs, lectures (21.2%), other methods (24.8%) such as social media, Workshops, Seminars, and collaboration between specialties (17.7%).
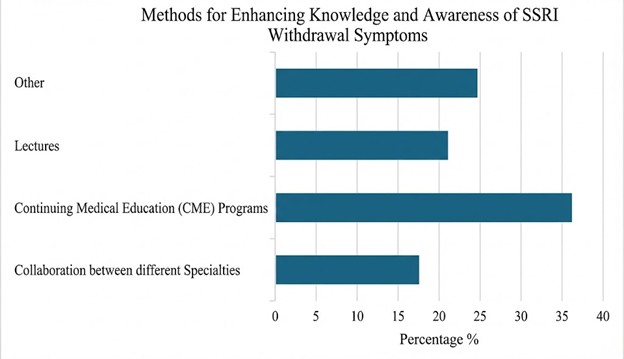
Figure 3: Distribution of the Suggested Methods by the physicians to enhance the Awareness and Knowledge of SSRI Discontinuation Effects
Table 4 presents the association between physicians' specialty and their reported encounters with patients experiencing discontinuation symptoms after abruptly stopping SSRIs. A significant difference was observed (p < 0.001), with psychiatrists far more likely to affirm such encounters (75.7%) compared to family medicine practitioners.
|
Table 4: Association between the Specialty of the physician and patients' experience of symptoms after suddenly stopping SSRIs |
||||
|
Factor |
Category |
Specialty N (%) |
P-Value |
|
|
Family Medicine |
Psychiatry |
|||
|
Have you encountered patients who have experienced discontinuation symptoms after abruptly stopping SSRIs? |
No |
35 (89.7) |
4 (10.3) |
0<.00*1 |
|
Yes |
18 (24.3) |
56 (75.7) |
||
|
*Chi-square test |
||||
Table 5 presents the associations between clinicians' years of clinical practice after graduation and their awareness of specific symptoms linked to SSRI discontinuation. Physicians reported differences in insomnia, nightmares, hypersomnia, and lethargy symptoms (p=0.003), with physicians with less than 6 years of experience demonstrating higher awareness (77%) than those with 6 years or more of experience.
|
Table 5: Association between the Years of clinical practice after graduation of the physician and their awareness of patients' experience of symptoms after suddenly stopping SSRIs |
||||
|
Factor |
Category |
Years of clinical practice after graduation N (%) |
P-Value |
|
|
≥ 6 years |
< 6 years |
|||
|
The symptoms you know are associated with SSRI discontinuation. |
||||
|
Anxiety, agitation, panic, depression, irritability, aggression, anger, and bouts of crying |
No |
4 (33.3) |
8 (66.7) |
0.751* |
|
Yes |
30 (29.7) |
71 (70.3) |
||
|
Balance problems, dizziness |
No |
8 (25.8) |
23 (74.2) |
0.542** |
|
Yes |
26 (31.7) |
56 (68.3) |
||
|
Insomnia, nightmares, hypersomnia, lethargy |
No |
14 (53.8) |
12 (46.2) |
0.003** |
|
Yes |
20 (23) |
67 (77) |
||
|
Other |
No |
1 (20) |
4 (80) |
<0.999* |
|
Yes |
33 (30.6) |
75 (69.4) |
||
|
*Fisher's Exact Test **Chi-square test |
||||
Discussion
Despite the generally favorable safety profile of SSRIs, the present results underscore the significant clinical burden of Antidepressant Discontinuation Syndrome (ADS) within local practice. In a retrospective chart review of 171 patients, withdrawal symptoms occurred in 17.2% patients, particularly those taking shorter half-life SSRIs (23). While recent systematic reviews estimate the true pharmacological incidence of withdrawal at approximately 15%, the prevalence of symptoms reported by patients in antidepressant treatment arms remains as high as 31% (11). Reflecting this substantial clinical reality, this study found that 57.4% of surveyed physicians in Riyadh have encountered patients experiencing withdrawal symptoms following abrupt cessation. Among those who observed these cases, the most frequently reported manifestations were emotional disturbances (71.6%) and flu-like symptoms (70.3%). These findings confirm that ADS is not merely a theoretical risk but a prevalent issue with substantial somatic and psychological impact in both primary and secondary care settings. The alignment between these local observations and international prevalence rates highlights the methodological reliability of the current survey in capturing real-world clinical challenges.
The primary finding of this study is the discrepancy between "active recall" and "passive recognition" of symptoms. When asked to list symptoms from memory, participants predominantly identified generic complaints such as headache (38.1%) and insomnia (31.0%), while specific features like anxiety were recalled by only 23.9%. However, when provided with a list, recognition rates spiked significantly: anxiety and emotional disturbances were recognized by 89.4%, insomnia by 77.0%, and balance issues like dizziness by 72.6%. This gap suggests that while physicians possess a latent knowledge of the syndrome, their spontaneous awareness is limited to non-specific symptoms. This mirrors the observation described in the diagnostic criteria proposed by Black et al. (7), in which dizziness and electric-shock sensations—hallmarks of ADS—are often overlooked unless specifically prompted (7). This lack of immediate recall contributes to diagnostic error; if a physician attributes a patient's dizziness or paresthesia to a new medical condition rather than withdrawal, it heightens the potential for misdiagnosis and polypharmacy. Importantly, these gaps in knowledge are now increasingly acknowledged by professional bodies and societies, reflecting a gradual shift in physician awareness of ADS (24).
The study also identified a significant disparity in awareness based on specialty and experience. Psychiatrists demonstrated markedly higher familiarity with discontinuation symptoms (95.2%) and were significantly more likely to report clinical encounters with ADS (75.7%) compared to Family Medicine physicians (24.3%). Furthermore, junior physicians (0–5 years of experience) were significantly more likely to recognize specific symptoms like insomnia (77%) compared to senior clinicians (>6 years), whose recognition rate was significantly lower at 23% (p=0.003). These results align with a survey from the United Kingdom, where psychiatrists were found to be nearly universally familiar with discontinuation events, whereas general practitioners lagged behind, as reported by Read et al. (15).
Similarly, a survey conducted by Khan et al. among physicians in Ireland demonstrated significant variability in the recognition and attribution of SSRI discontinuation symptoms across different levels of training, with less experienced doctors attributing fewer symptoms to SSRIs and general practitioners often generalizing these effects across antidepressant classes (26).
This divergence likely stems from the training background; 71.7% of respondents acquired their knowledge primarily through residency and clinical experience rather than medical literature (23.0%). Since psychiatrists manage long-term maintenance and tapering more frequently, they gain this experiential knowledge, whereas family physicians may inherit these patients without the specialized practical exposure required for deprescribing. This creates a practical gap; previous observational studies indicate that even when tapering strategies are attempted in routine clinical practice, they often differ from guidelines, and patients frequently experience symptoms despite gradual dose reduction (20).
Regarding patient management, the therapeutic alliance relies heavily on transparent communication. It is therefore concerning that while the majority of respondents educate patients "always" (38.1%) or "often" (31.9%), 30% of participants reported doing so inconsistently, specifically "sometimes" (22.1%), "rarely" (4.4%), or "never" (3.5%). This finding is consistent with previous survey-based research by Read and Williams, in which 1431 antidepressant users from 38 countries reported their experiences; one-third indicated they had not been informed about any side effects by their prescriber, and fewer than 5% recalled being warned about critical issues such as suicidality or withdrawal effects (25). Literature from a mixed-method study by Guy et al. (21) indicates that failure to warn patients about potential withdrawal effects is a leading cause of non-adherence, while a chart review found that patients who experience unexpected somatic symptoms often discontinue treatment abruptly, creating a cycle of relapse and withdrawal (22).
To address these deficits, participants expressed a clear preference for structured learning. CME programs were the most favored intervention (36.3%), followed by workshops and seminars (24.8%), lectures (21.2%), and collaboration between specialties (17.7%). This indicates that physicians are aware of their knowledge gaps and are receptive to training that focuses specifically on tapering protocols and symptom recognition. In light of these preferences, future efforts might arguably benefit from the adoption of broad supportive categories rather than isolated tools. For example, the integration of point-of-care clinical decision support systems could serve to reinforce symptom recognition at the time of consultation, effectively bridging the gap between latent knowledge and active clinical application.
Strengths and Limitations
Although the study benefits from a well-balanced sample of family physicians and psychiatrists, enhancing the reliability and representativeness of the prevalence data. And addresses a clinically relevant issue that has direct implications for everyday practice. Several limitations should be considered. First, the study includes only physicians in family medicine and psychiatry, excluding other relevant specialties (e.g., neurology, internal medicine). This may limit the breadth of perspectives on SSRI discontinuation symptoms. Second, the sample includes physicians from Riyadh City only, with a heavy predominance of public-sector physicians. This limits the ability to generalize findings to physicians in other regions or to private-sector clinicians. The third limitation is that the findings rely entirely on self-reported data from physicians, which introduces potential recall bias and social desirability bias, as participants may overestimate their familiarity or underreport uncertainty. Finally, the cross-sectional design captures physician awareness at a single point in time and does not allow for assessment of changes in knowledge or practice over time.
Future Directions
Future research should expand to include other specialties that prescribe antidepressants, such as internal medicine and neurology, to obtain a comprehensive view of prescribing practices. Additionally, longitudinal studies assessing the impact of specific educational interventions would be valuable. Lastly, further research is needed to assess awareness among physicians in different cities throughout the Kingdom.
Conclusion
This study establishes Antidepressant Discontinuation Syndrome as a prevalent clinical reality in Riyadh, characterized by fragmented physician awareness. The critical disconnect between passive recognition and active recall, combined with significant specialty-based disparities, highlights a vulnerability in primary care. As the healthcare system integrates mental health services, these findings necessitate the development of clinical decision support tools and structured educational interventions.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding.
Ethical consideration
This study was approved by the Institutional Review Board (IRB) at King Abdullah Bin Abdulaziz University Hospital (Log Number: 25-0002) on January 28, 2025.
Data availability
All data are available within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.