Volume 5, Issue 12
December 2025
Infection Control Strategies in Maxillofacial Traumas and Prevention of Complications
Ziyad Abdulaziz AlHammad, Alaa Hussin Bosaleh, Abdullah Khalaf Alghamdi, Abdulbari Mohammed Aleidan, Sultan Saeed Alqahtani, Mona Abdulmohsen Alsoli
DOI: http://dx.doi.org/10.52533/JOHS.2025.51212
Keywords: Maxillofacial trauma, infection control, fracture-related infection, surgical site infection, antibiotics prophylaxis
Maxillofacial trauma is a serious issue that imposes a huge burden on healthcare systems worldwide. Etiology of maxillofacial trauma varies, with road traffic accidents being the most common cause. Its incidence varies between countries due to multiple factors, especially socioeconomic factors. Infection is a common complication for maxillofacial trauma, given the rich bacterial environment of this area. This infection can significantly worsen postoperative outcomes that may require more complex interventions. Types of maxillofacial trauma infection involve fracture-related infection (FRL) and surgical site infection (SSI), both of which can be prevented by infection control strategies. Various infection control strategies for maxillofacial surgeries were developed; however, the variability in infection control methods led to mixed results. This review aims to explore current evidence about infection control strategies in maxillofacial trauma and its effectiveness in reducing infection rates. Infection rates in maxillofacial trauma vary with mandibular fractures showing the highest infection rate. Antibiotic prophylaxis is the main infection control method, which showed effectiveness if it was administered within the first 24 hours following surgery, as exceeding this period has shown no additional benefits. Infection control strategies should consider risk factors, such as comorbidities and surgical factors. Future studies should focus on establishing harmonized guidelines based on robust data for infection control in maxillofacial trauma.
Introduction
Maxillofacial trauma represents a considerable burden on healthcare systems all over the world. Its incidence varies widely due to the socioeconomic differences between countries. The etiology of maxillofacial trauma includes road traffic accidents (RTAs), interpersonal violence, and falls. It is associated with various complications, such as fractures, hemorrhage, nerve injury, and infection. Infection in maxillofacial trauma represents more burden on healthcare systems. Surgery of maxillofacial injuries can be associated with postoperative infection, which may be presented as fracture-related infection (FRI) or surgical site infection (SSI) (1, 2). These infections may result in prolonged hospitalization, increased morbidity, and adverse clinical outcomes, such as nonunion of fractures and chronic osteomyelitis (3).
Fracture-related infection is defined as the occurrence of infection due to a bone fracture, which can arise regardless of whether surgical intervention is performed (4). This type of infection differs from other types of musculoskeletal infection, as it is susceptible to biomechanical instability and is associated with frequent involvement of soft tissue and potential vascular damage (1). Thus, it is associated with a poor healing process and increased risk of postoperative infection. FRI can be in the form of mild conditions, such as plate exposure without associated clinical manifestations, or in the form of severe cases presenting with nonunion with osteomyelitis, and abscess formation (1). FRI’s incidence in maxillofacial trauma varies widely due to factors such as patient demographics, fracture type, and surgical approach (5). Reports of its incidence were up to 20% across the literature (1). Risk factors for postoperative FRI include patient-related factors, such as comorbidities like diabetes mellitus, smoking, and substance abuse, and surgical factors, such as the complexity and severity of the fracture, fixation method, and the timing of intervention (6, 7).
Surgical site infection is the occurrence of infection either within the first 30 days following surgery or during the first year following the placement of foreign material (8). This type of infection commonly occurs in cases of maxillofacial trauma given the omnipresent bacterial flora of the oral and nasal cavity. The incidence of SSI in maxillofacial trauma is between 0% and 30%, with an average of 12% (9). Comorbidities, such as diabetes and obesity, and surgery-related factors, such as duration of surgery and hospital stay, are among major risk factors for SSI following maxillofacial trauma surgery (8, 10).
Prevention of infection in maxillofacial trauma is critical to improve postoperative clinical outcomes and reduce the burden on healthcare systems. Multiple infection control strategies have been introduced by previous studies. These strategies are mainly based on antibiotic prophylaxis, but they also may include preoperative periodontal health and oral hygiene assessment, topical skin antiseptics, debridement and soft tissue management, and local antimicrobial therapy. However, a universal strategy for infection control in maxillofacial injuries is still unavailable, due to the variability in infection control methods and in antibiotic selection and duration across studies. This review aims to investigate strategies for infection control in maxillofacial trauma introduced by current evidence, highlighting the role of antibiotic prophylaxis.
Methods
A comprehensive literature search was conducted in Medline (via PubMed), Scopus, and Web of Science databases up to September 25, 2025. Medical Subject Headings (MeSH) and relevant free-text keywords were used to identify synonyms. Boolean operators (AND’, OR’) were applied to combine search terms in alignment with guidance from the Cochrane Handbook for Systematic Reviews of Interventions. Key search terms included: “Maxillofacial trauma” AND “Infection control”. Summaries and duplicates of the found studies were exported and removed by EndNoteX8. Any study that discusses infection control strategies in maxillofacial traumas and published in peer-reviewed journals was included. All languages are included. Full-text articles, case series, and abstracts with the related topics are included. Case reports, comments, and letters were excluded.
Discussion
Overview of Maxillofacial Trauma
The epidemiology of maxillofacial trauma varies globally due to socioeconomic, cultural, and environmental factors (11). It accounts for 33-55% of trauma cases and approximately 15% of all emergency department visits globally (12). High-income countries have shown reduced incidence of maxillofacial trauma in recent years, while low- and middle-income countries still show high incidence, mainly due to road traffic accidents, inadequate infrastructure, and limited enforcement of safety regulations (13, 14). The highest incidence of maxillofacial trauma is noticed in young adult males (20-40 years) due to increased risk of RTAs and interpersonal violence among this age group (14). In old age, this gender disparity reduces, as falls become the predominant cause (15). Socioeconomic status, alcohol, and substance abuse are major contributing factors for maxillofacial trauma (16, 17). Furthermore, the severity of injuries varies according to the setting, with urban areas showing more severe, high-velocity trauma compared to lower-velocity injuries common in rural areas (18).
The etiology of maxillofacial trauma also varies significantly across geographical regions. Globally, RTAs are considered the most common cause of maxillofacial injuries. Mijiti et al. reported that RTAs account for 61.5% of maxillofacial fractures, with developing countries showing 2.7 times higher rates than developed countries (19), reflecting insufficient structure, inadequate traffic regulations, and poor implementation of safety measures. Interpersonal violence is another major cause of maxillofacial injuries, while classifying domestic violence as a major cause is challenging due to underreporting and intervention difficulties (20). Falls are a common cause of maxillofacial injuries, particularly among older populations (21). Furthermore, falls and playground accidents are common causes in pediatric populations, which require specialized management approaches due to the developing facial skeleton (22). Sports-related and occupational accidents also contribute to the etiology of maxillofacial injuries (23, 24). Other etiologies have emerged due to emerging lifestyle trends, such as injuries from personal mobility devices like electric scooters and accidents related to distracted walking or driving due to mobile device use (14). Epidemiology of maxillofacial trauma is shown in Figure 1.
Maxillofacial trauma may involve soft tissues, hard tissues, or dentition of the face, or a combination of them. It has been reported that soft tissue injuries occur in 78.6% of maxillofacial trauma cases, with lacerations being the most common (53.2%), followed by contusions (22.9%) and abrasions (15.8%) (12). Facial fractures also commonly occur following maxillofacial trauma, with mandibular fractures being the most common facial bone injuries. Facial fractures can also involve condylar fractures, midface fractures, and nasal bone fractures. The extent of facial fractures is determined by mechanism, impact force, and intrinsic bone strength (25). Furthermore, maxillofacial trauma is frequently associated with dental trauma, ranging from uncomplicated crown fractures to complete tooth avulsion (14). Maxillofacial trauma can lead to injuries of related structures, such as traumatic brain injuries (26), cervical spine injuries (27), ocular trauma (28), and airway compromise (29), which necessitates comprehensive assessment.
Maxillofacial trauma represents a significant burden on the healthcare systems worldwide. The complex nature of this type of trauma and the multidisciplinary approach required for its management are associated with high, direct healthcare costs, and these costs play a crucial role in shaping health system budgets (30).
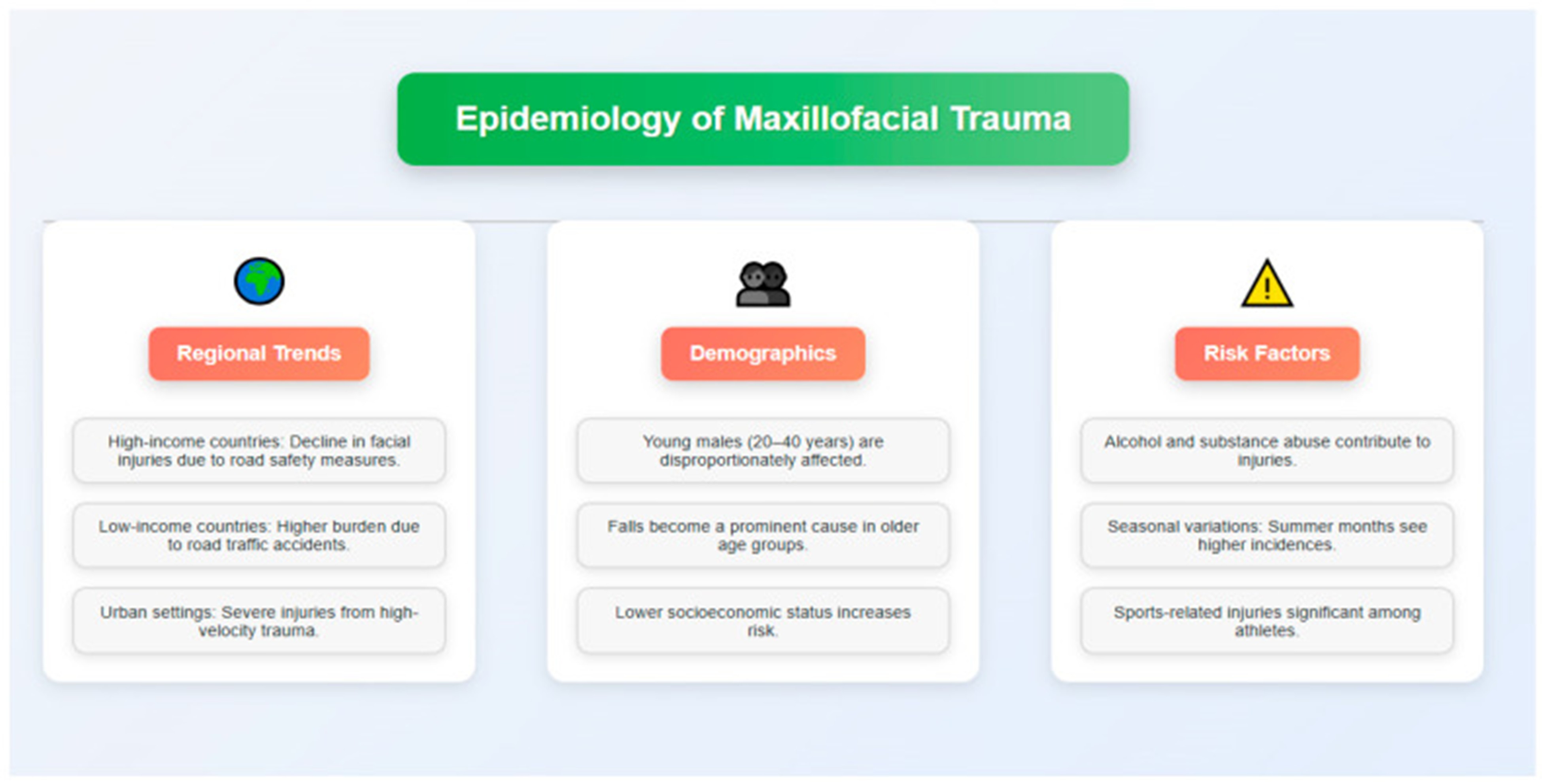
Figure 1: Epidemiology of maxillofacial trauma (14)
Infection in Maxillofacial Trauma
Maxillofacial trauma is associated with various mechanisms of infection, including fracture-related infections and surgical site infections (1, 2). These infections may result in prolonged hospitalization, increased morbidity, and adverse clinical outcomes, such as nonunion of fractures and chronic osteomyelitis (3). A recent systematic review and meta-analysis by Cruyssen et al. reported an overall pooled maxillofacial fractures-related infection rate of 5.6%, with mandibular fractures showing the highest infection rate (8.9%), followed by frontal bone fractures (2.7%), condylar fractures (1.8%), and midface fractures (0.9%) (1). Multiple risk factors for FRIs following maxillofacial trauma were reported in previous studies. Smoking is a major risk factor, as it has been associated with higher complication rates and higher risk of osteosynthesis-related infections (31). Substance abuse, including alcohol abuse and intravenous drug abuse, has also been associated with higher complication rates, higher infection rates, malunion, and other postoperative complications (32).
Increasing age and comorbidities, such as diabetes mellitus, increase the risk of FRIs following maxillofacial trauma, as these patients have decreased bone density, impaired immune function, and multiple comorbidities that hinder the healing process, increasing the risk of infection (33, 34). Furthermore, surgical techniques and fixation methods can significantly impact maxillofacial fracture-related infection rates. Studies showed that intraoral surgical approaches have been associated with increased rates of postoperative infection (31, 35), while no significant differences were observed between fixation methods (35, 36). The role of prophylactic antibiotics as a risk factor for maxillofacial FRIs has been examined. Andreasen et al. showed that antibiotic administration lowered infection rates to 7% compared with no antibiotics and that a single dose could be as effective, or even superior, to a prolonged regimen (37).
Infection Control Strategies in Maxillofacial Trauma
Infection control in maxillofacial trauma is critical to improve clinical outcomes and reduce its burden on healthcare systems. Multiple studies have discussed prevention of FRI and SSI strategies in various settings. These strategies included perioperative antibiotic prophylaxis, topical skin antiseptics, debridement and soft tissue management, and local antimicrobial therapy (38). Both animal and human studies reported that perioperative antibiotic prophylaxis reduced the risk of postoperative infection and that it should be administered as early as possible (39, 40). In case of closed fracture, a single dose of antibiotic, with gram-positive coverage, one hour prior to surgical incision is recommended (41, 42). Notably, antibiotic administration is only recommended in cases of closed fracture that require surgical procedure (43). On the other hand, the type and duration of antibiotic administration in open fractures are determined by the severity of injury. However, uniformly accepted guidelines regarding antibiotic administration in open fractures are still lacking (44).
In 1867, Lister highlighted the importance of using carbolic acid as a topical skin antiseptic at the time of surgery to reduce the risk of postoperative infection (45). Currently, the most used topical skin antiseptics include povidone-iodine, alcohol, or chlorhexidine-gluconate. However, it should be noted that these antiseptics may result in local toxicity to deeper tissues in cases of open fractures (46). Furthermore, an extensive debridement of all non-healthy tissues and foreign bodies is essential to avoid any postoperative infection. Previously, it was advised that debridement should be performed as urgently as possible; however, subsequent studies have not supported this concept, highlighting the importance of adequacy over urgency (41). The use of local antimicrobial therapy in preventing FRIs has been emerging in the last decades. A previous meta-analysis found that the use of local antibiotic therapy was associated with an 11% postoperative infection risk reduction when compared with conventional treatment (47). However, this finding still requires support from further studies.
Antibiotic Prophylaxis in Maxillofacial Surgeries
In maxillofacial trauma surgeries, it has been reported that the infection rate can be significantly reduced through the administration of a single preoperative dose followed by 24-48 h of postoperative antibiotics. Andreasen et al. reported that infection rates were reduced by 7% following antibiotic prophylaxis for maxillofacial fractures and that a single dose may be just as effective, or even more so, than an extended course (37). Supporting this finding, Mottini et al. (48) and Blatt and Al-Nawas (49) found that an extended course (5 days or more) of surgical antibiotic prophylaxis in maxillofacial fractures did not show any significant benefits in preventing SSIs over a 1-day postoperative course of surgical antibiotic prophylaxis. Shridharani et al. advised against the extended use of antibiotic prophylaxis (beyond 24 hours) in patients with mandibular fractures (50), while Bartella et al. reported that single-shot antibiosis is sufficient for prophylaxis against SSIs following maxillofacial surgeries (51). In their systematic review, Milic et al. recommend the administration of postoperative antibiotics (not exceeding 24 h) in mandibular fractures, while in upper/midface fractures, postoperative antibiotics are not recommended (52).
Furthermore, Habib et al. reported that the use of postoperative surgical antibiotic prophylaxis, no matter the duration, had no significant impact on reducing the risk of SSI following facial fracture surgery (53). Therefore, they did not recommend the routine use of postoperative antibiotics in this setting. They also recommended individualized strategies of antibiotic prophylaxis according to the patient’s health status, mechanism of injuries, and osseous and soft tissue condition. Interestingly, Delaplain et al. found that extended postoperative antibiosis in cases of mandibular fractures was paradoxically linked to a higher risk of SSI (54). According to the current Surgical Infection Society (SIS) guidelines, postoperative antibiotic administration beyond 24 hours is not recommended for adults with midfacial or mandibular fractures (55).
The routine use of preoperative antibiotics has also been evaluated by previous studies. Linkugel et al. opposed the routine administration of antibiotics in the interval between injury and surgery, as they found that preoperative antibiotic administration may increase the risk of SSIs (56). Zosa et al. also found that prolonged administration of preoperative antibiotics in patients with facial fractures did not decrease the incidence of SSIs (57). The latest SIS guidelines support the avoidance of prescribing preoperative antibiotics in cases of facial fractures (55). However, variability in antibiotic selection and duration across studies suggests a need for consensus guidelines to optimize prophylactic strategies and minimize the development of antibiotic resistance.
Clinical Implications
Perioperative antibiotics prophylaxis is the mainstay component in infection control strategies for maxillofacial trauma. Preoperative antibiotic prophylaxis is not recommended, since it does not reduce infection rate; in fact, it may increase the risk. Administration of postoperative antibiotics should not exceed the first 24 hours following surgery, as exceeding this period adds no benefits. Adequate soft tissue management should be done through the debridement of any unhealthy tissues. Local antiseptics and local antimicrobial therapy can significantly reduce postoperative infection rates. Individualized infection control strategies should be adopted based on patient-related factors, such as comorbidities, and surgery-related factors, such as duration and type of surgery.
Conclusion
Infection in maxillofacial trauma is a huge burden on healthcare systems that require multidisciplinary strategies to reduce its risk. While postoperative antibiotic prophylaxis should be confined to the first 24 hours following surgery, preoperative prophylaxis is not recommended. Soft tissue management, local antiseptics, and local antimicrobial therapy should be integrated into future strategies for infection prevention in maxillofacial surgeries. Future studies should focus on developing clinical guidelines based on robust data for infection control in maxillofacial trauma.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding.
Ethical consideration
Non applicable.
Data availability
Data that support the findings of this study are embedded within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.
