Volume 5, Issue 11
November 2025
Clinical Outcomes of Apexification Techniques in the Management of Immature Teeth
Muhannad Talal Shuman, Walaa Talal Fatani, Mohammed Ali Alfadaghem, Hawra Hameed Alobaid, Fatimah Abdullah Alqahtani
DOI: http://dx.doi.org/10.52533/JOHS.2025.51110
Keywords: Immature teeth, Apexification, Calcium hydroxide, Mineral trioxide aggregate, Regenerative endodontic therapy
Immature teeth are developing permanent teeth with incomplete root formation, characterized by an open apex, thin dentinal walls, and underdeveloped root length. It results from pulp necrosis that may be caused by dental trauma, dental caries, or apical periodontitis. Apexification has been the treatment of choice for immature teeth for years. Apexification techniques include apexification with calcium hydroxide and apexification with apical plug using mineral trioxide aggregate (MTA) or biodentine and other bioceramics. Regenerative endodontic therapy is another treatment option for immature teeth. These treatment modalities are associated with various success rates and various clinical outcomes. This review aims to evaluate clinical outcomes of different apexification techniques in the management of immature teeth. Apexification aims to resolve symptoms of periapical disease, heal periapical lesions radiographically, and form a calcified tissue barrier at the apex. Long-term calcium hydroxide apexification has been used for years; however, it involves disadvantages, such as long treatment duration and high risk of contamination. The apical plug technique has become preferred by clinicians due to its short treatment duration and favorable clinical outcomes, especially with Bodentine, which does not lead to tooth discoloration, unlike MTA. Regenerative endodontic procedures have shown similar overall success and survival to apexification, but better root length and dentin wall thickness. Future studies should focus on comparing success rates, clinical outcomes, and safety of different treatment modalities for immature teeth based on large population studies.
Introduction
After eruption of the tooth, complete root development and apex closure typically occur within 3 years (1). Immature teeth are newly erupted teeth with open apices that can normally be closed after 3 years of tooth eruption (2). Clinicians find difficulty in managing this condition, especially in instrumentation, determination of working length, and control of irrigants and obturation materials, as these teeth are characterized by open apices, thin dentinal walls, and very wide canals (3). Furthermore, immature teeth are more susceptible to fracture; therefore, even with optimal endodontic treatment, their long-term prognosis remains unfavorable (4). Immature teeth may result from dental trauma, dental caries, or periapical periodontitis, all of which lead to pulp necrosis, resulting in the arrest of root development of immature teeth. Dental trauma injuries account for 30% of pulpal necrosis on an immature permanent tooth (5, 6).
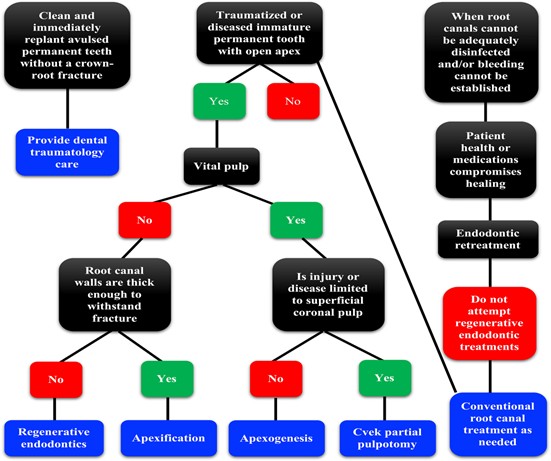
Treatment options for immature teeth depend on pulp vitality; apexogenesis is recommended for vital teeth, and apexification is recommended for non-vital teeth (Figure 1) (7). Apexification is the induction of calcified barrier formation at the root with open apices or the ongoing apical root development in immature teeth with necrotic pulps (8). It aims to create an apical barrier, which can enhance the root canal obturation procedure and prevent the extrusion of root canal filling material into the periapical zone (9). For years, long-term apexification using calcium hydroxide has been the treatment of choice for immature teeth. However, this material is associated with various limitations, such as multiple clinic visits, long treatment duration, and high risk of infection recurrence and fracture (10, 11).
The placement of an apical plug using mineral trioxide aggregate (MTA) has been developed as an alternative to apexification with calcium hydroxide (12). MTA apexification has been associated with favorable outcomes comparable to those of long-term calcium hydroxide apexification outcomes (13). Although it leads to fewer clinic visits, MTA apexification was associated with unimproved root strength and tooth discoloration (14). BiodentineTM, which is a tricalcium silicate-based material similar to MTA, has been developed to overcome MTA shortcomings (11). It offers handling advantages, biocompatibility, and the ability to induce hard tissue formation, making it a promising substitute for MTA (11). Biodentine has been used in various dental procedures, such as direct restorative posterior filling, retrograde restoration, indirect and direct pulp capping, apexification, apexogenesis, and regenerative endodontic therapy (15).
Regenerative endodontic therapy is another treatment option for immature teeth, showing comparable favorable outcomes as apexification (16). Although it led to similar overall success and survival rates as apexification, regenerative endodontic therapy showed better root development, as observed in increased root length or increased dentinal wall thickness (17). Nevertheless, studies reported that endodontists mainly prefer apexification due to its evidence-based foundation and predictable treatment outcome, as well as patient compliance, a well-established number of required patient visits, and a known likelihood of tooth discoloration (18).
Multiple treatment options for immature teeth are available with variable effectiveness and variable advantages for each option over the other, which necessitates a thorough comparison between all options in terms of success rates, survival rates, clinical outcomes, and safety. This review aims to evaluate clinical outcomes of different apexification techniques in the management of immature teeth, highlighting the advantages and shortcomings of different materials that can be used in the apexification procedure. It also aims to explore the use of regenerative endodontic therapy in the management of immature teeth and to compare it with apexification.
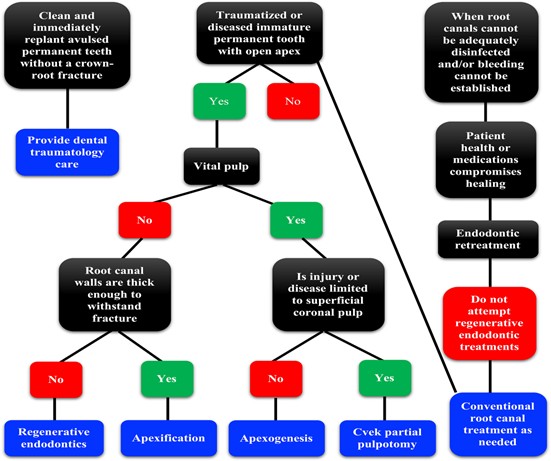
Figure 1: Flow chart for selecting appropriate endodontic treatments for immature teeth (19).
Methods
A comprehensive literature search was conducted in Medline (via PubMed), Scopus, and Web of Science databases up to October 8, 2025. Medical Subject Headings (MeSH) and relevant free-text keywords were used to identify synonyms. Boolean operators (AND’, OR’) were applied to combine search terms in alignment with guidance from the Cochrane Handbook for Systematic Reviews of Interventions. Key search terms included: “Apexification” AND “Immature teeth”. Summaries and duplicates of the found studies were exported and removed by EndNoteX8. Any study that discusses clinical outcomes of apexification techniques in the management of immature teeth and published in peer-reviewed journals was included. All languages are included. Full-text articles, case series, and abstracts with the related topics are included. Case reports, comments, and letters were excluded.
Discussion
Overview of Immature Teeth and Apexification
Pathologically immature teeth may result from trauma, which leads to pulp necrosis, resulting in the arrest of root development of permanent immature teeth (20). These immature pulpless teeth retain an open apex with thin, short root walls (21). Pathologically immature teeth may also occur due to apical resorption due to trauma, or chronic periapical periodontitis, mechanical debridement-induced destruction of apical constriction, apicoectomy without use of root-end filling materials, and horizontal root fracture (22, 23).
Apexification is one of the most popular treatment methods for open apex immature teeth. Apexification techniques include apexification with calcium hydroxide and apexification with the placement of artificial apical barriers at the blunt apex (20). Artificial apical barriers can be made from various materials, such as MTA, biodentine, and a calcium-enriched mixture. Apexification aims to resolve symptoms of periapical disease, heal periapical lesions radiographically, and form a calcified tissue barrier at the apex (20).
Apexification Techniques
Calcium Hydroxide Apexification Technique
This technique involves the placement of calcium hydroxide in the root canal for a period of time to induce the formation of a hard-tissue apical barrier that leads to root canal obturation, preventing the passage of toxins and bacteria into the periapical tissues (24). A calcified apical barrier is formed and consists of an outer acellular cementum-like layer and a central fibrocollagenous connective tissue core (25). However, the extended use of calcium hydroxide can lead to reduced fracture resistance of root dentine (26). Furthermore, extended use and the difficulty of monitoring patients are additional challenges that necessitate the development of alternatives (27). It has been reported that calcium hydroxide remained in the root canal for up to 12 months in 59% of the relevant clinical studies and up to 24 months in 10% of the other studies (20).
In addition, the frequency and number of calcium hydroxide changes have been investigated. Some studies reported that the use of intracanal medicament can be effective alone in inducing a hard-tissue apical barrier (28), while others found that multiple changes of calcium hydroxide are associated with better outcomes, such as quicker induction of the apical bridge (29). It has been reported that 85% of related studies reported two or more replacements of that intracanal medicament, indicating that clinicians preferred replacing calcium hydroxide at least twice to achieve the desired outcome. Bezgin et al. have examined the use of Calcium Hydroxide-Polyethylene Glycol Paste (CHPP) as an alternative to calcium hydroxide paste for use as intracanal medication(30). CHPP has shown effectiveness in the treatment of cases where apexification with calcium hydroxide is indicated. Another study by Oktem et al. used CHPP tips in a tooth with a 24-month follow-up, which demonstrated successful apex closure (31).
Apical Plug Apexification Technique
This technique uses an artificial barrier, made of MTA, biodentine, or a calcium-enriched mixture, to form an artificial seal that allows for the proper compaction of gutta-percha against it. Unlike long-term calcium hydroxide apexification, apical plug apexification can be completed in one visit without the use of an intracanal medicament (32) or in two or more visits with the use of medication (3, 33). Notably, calcium hydroxide can be used as an intracanal medicament for intracanal disinfection in the orthograde apical plug technique.
Multiple studies have evaluated the use of MTA as an alternative to achieve root closure in immature teeth or root fracture (34-36). The formation of a barrier using MTA requires significantly less time than using calcium hydroxide. Mente et al. examined apexification treatment in a large sample with a 10-year follow-up period and found that MTA is an effective option for teeth with an open apex (37). They identified preoperative apical periodontitis as the most important prognostic factor for the success of apexification. Furthermore, Chang et al. investigated the effect of MTA on apexification and periapical scarring, especially in cases of MTA extrusion (38). They found that MTA extrusion through an open apex has no negative impact on the healing of the periapical tissues. Yadav et al. examined a one-visit apexification using MTA combined with a platelet-rich fibrin apical plug (PRF) (39). PRF is easily prepared and lacks biochemical modification of the blood, which makes this preparation strictly autologous. It also involves an increase in cytokine and leukocyte levels, which function as anti-inflammatory and anti-infective agents, regulate immune responses, and supply vascular endothelial growth factor to stimulate angiogenesis (39).
Biodentine and other bioceramic materials were developed to overcome the shortcomings of MTA in apexification treatment (11). The use of biodentine and ceramics in apexification is associated with more rapid and effective outcomes compared to other materials. A recent case report reported a case of an immature tooth due to trauma, which was treated with an apical plug made of calcium silicate-based bioceramic cement, namely BIO-C ® Repair (40). The patient showed gradual progress in healing as shown by the increase in the density of the alveolar bone at the apical of tooth (40). This material has a major advantage, which is the ability to modify its composition, particle size, and preparations in order to correct the deficiencies of previous MTA materials, such as ProRoot MTA and MTA Angelus. Notably, it is important to replace the bismuth oxide composition, which functions as a radio-opacity material, with zirconium oxide to prevent tooth discoloration (40).
Another advantage of calcium silicate-based bioceramic cement is its small particle size, which increases the surface area, resulting in a faster hardening time compared to MTA material. The particle size of ProRoot MTA is 5-19 μm, with an initial setting time of 40 minutes and a final setting time of 4 hours (41, 42), while BIO-C ® Repair has a particle size of 2 μm, an initial setting time of 15 minutes, and a final setting time of 2 hours. Meanwhile, BiodentineTM has the fastest setting time, with an initial setting time of 6 minutes and a final setting time of 10-12 minutes, which is attributed to the content of calcium chloride accelerator in the liquid (43).
A recent review of studies and case reports assessed the use of BiodentineTM in apexification of immature teeth (11). Previous case reports have reported various preoperative symptoms and signs, including swelling, pain, discoloration, fracture, pain on percussion and palpation, presence of sinus tract, discharge of pus, and radiolucent lesions in the periapical area. BiodentineTM has been associated with positive clinical outcomes, including reduced swelling and pain, resolution of pus and sinus tracks, no discoloration, and improved function and aesthetics of the restored tooth. It has also been associated with better radiographic outcomes, including healing of periapical radiolucent lesions, regeneration of periradicular tissues, continued root development, formation of a calcified apical barrier, thickening of the apical dentin wall, and elongation of the apical root (10, 44). Differences between calcium hydroxide apexification and apical plug apexification are summarized in Table 1.
|
Table 1. Comparison Between Calcium Hydroxide Apexification and Apical Plug Apexification (20, 45) |
||
|
Calcium Hydroxide Apexification |
Apical Plug Apexification (MTA/Biodentine) |
|
|
Treatment duration |
Long (months to years; multiple visits) |
Short (single or two visits) |
|
Mechanism |
Induces the biological formation of a calcified apical barrier |
Creates an artificial apical barrier using bioactive material |
|
Root strength |
Decreased with long-term use due to dentin brittleness |
Preserved or improved |
|
Handling properties |
Easy to place but requires frequent replacement |
MTA: difficult handling, Biodentine: improved workability |
|
Tooth discoloration |
Minimal |
Common with MTA (due to bismuth oxide); absent with Biodentine |
|
Risk of reinfection |
Higher (long-term canal exposure) |
Lower (short treatment time) |
|
Main advantages |
Cost-effective, long clinical history |
Fast, reliable barrier formation, fewer visits |
|
Main disadvantages |
Long duration, root weakening, risk of contamination |
Higher material cost, technique-sensitive manipulation |
Regenerative Endodontic Therapy versus Apexification
A systematic review and meta-analysis by Pendse et al. aimed to compare the effectiveness of regenerative endodontic procedures (revascularization) and apexification with MTA in young human immature nonvital teeth (46). Outcomes included root length, canal width, apical diameter, dentinal wall thickness, and canal morphology. They found that revascularization was associated with higher root length and width; thus, it is more effective than MTA apexification in promoting root maturation (47). This is especially crucial in young patients, as long-term tooth survival relies on ongoing root maturation and reinforcement of the dentinal walls (48). Revascularization also showed better apical closure and radicular dentin, as well as regenerative capacity, compared to MTA apexification (49, 50). Pendse et al. concluded that both treatment options are effective for immature nonvital teeth; however, revascularization seems to provide greater potential for promoting further root development and enhancing structural reinforcement (46).
Another systematic review and meta-analysis by Stefanidou et al. evaluated the long-term outcomes of immature teeth in terms of root length and dentin wall thickness when treated with apexification compared to regenerative endodontic procedures (revitalization) treatment (51). Revitalization is a procedure aimed at generating new pulp-like tissue within the root canal to restore pulp vitality and reduce the risk of tooth loss (52). The study found that revitalization was associated with a more significant increase in both root length and dentin wall thickness in all included studies, while apexification procedures led to minor improvement in root length (47, 53, 54). In fact, it was not associated with any improvement in root dentin wall thickness in some studies (47, 53, 54). Notably, it has been reported that the age of the patient is correlated with the success of these procedures, as stem cells of younger patients have a higher potential for regeneration when compared to the stem cells of older patients (55).
Furthermore, Tewari et al. compared the effectiveness of regenerative endodontic treatment to apexification in the management of necrotic immature permanent teeth with or without apical periodontitis (17). The study reported no significant difference in overall success and survival between the two treatment options, which indicates that both treatments are effective in treating necrotic immature permanent teeth with or without apical periodontitis (17). However, they found that regenerative endodontic treatment was associated with higher radicular dentinal wall thickness and root length.
Clinical Implications
Apexification techniques for the management of immature teeth include the calcium hydroxide apexification technique and the apical plug apexification technique (MTA and biodentine and other bioceramic apexification). Long-term calcium hydroxide has been used for apexification of immature teeth for years; however, apical plug apexification has been preferred in recent years. Advantages of apical plug apexification over calcium hydroxide include short treatment duration, single-visit procedure, reduced microleakage, and faster apical barrier formation. Despite these advantages, studies showed that calcium hydroxide apexification may be associated with higher rates of apical closure, which may reflect its biological mechanism of promoting hard tissue formation and long-term preservation of treated teeth. Overall, both techniques lead to favorable outcomes, with the apical plug technique being preferred due to its short treatment duration.
Materials used for apical plug apexification include mineral trioxide aggregate, biodentine and other bioceramic materials. When comparing them, mineral trioxide aggregate has various shortcomings, such as difficult manipulation and insertion, long setting time, tooth discoloration, and release of heavy metal substances such as arsenic (10). On the other hand, biodentine was developed to overcome these shortcomings, as observed in its faster setting time and its ability to eliminate the potential for tooth discoloration. Biodentine offers handling advantages, biocompatibility, and the ability to induce hard tissue formation, making it a promising substitute for MTA and apexification in future apexification protocols. Regenerative endodontic procedures have been emerging in the treatment of immature teeth. It has shown similar overall success and survival similar to apexification; however, regenerative endodontic procedures were found to achieve better root length and dentin wall thickness. Thus, it could, overtime, replace apexification as the treatment of choice for immature teeth.
Conclusion
Apexification techniques in the management of immature teeth include apexification with the calcium hydroxide technique and apexification with the placement of the apical plug technique using different materials, such as mineral trioxide aggregate and biodentine. Both techniques achieve favorable clinical and radiographic outcomes; however, apexification with apical plug is associated with fewer visits and no tooth discoloration, making it preferable for the treatment of immature teeth. Regenerative endodontic therapy achieves similar overall success rates but more improvement in root health; thus, it may become the treatment of choice for immature teeth in the future. Future studies should focus on comparing success rates, clinical outcomes, and safety of different treatment modalities for immature teeth based on large-population studies.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding.
Ethical consideration
Non applicable.
Data availability
Data that support the findings of this study are embedded within the manuscript.
Author contribution
All authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.