Volume 6, Issue 6
June 2026
Maxillary Second Molar with Two Separated Palatal Roots: A Case Report
Wafa Mansour Alqahtani
DOI: http://dx.doi.org/10.52533/JOHS.2026.60602
Keywords: obesity, Maxillary second molar, separated palatal roots, root canal, symptomatic irreversible pulpitis, apical periodontitis, CBCT
Background: The normal anatomy of the second maxillary molar consists of three roots: mesiobuccal root, distobuccal root, and palatal root. However, there are several variations in the anatomy of the root canal system of the second maxillary molar, such as the presence of four canals: two buccal and two palatal canals.
Case Presentation: We present a rare case of 60-year-old male with no medical history presented with a deep carious lesion in the occluso-mesial surface of the left second maxillary molar. The preoperative diagnostic radiograph depicted periapical radiolucency surrounding the distobuccal root and a variation in the morphology of the number of roots and root canals: four roots, including two palatal roots. A diagnosis of symptomatic irreversible pulpitis and symptomatic apical periodontitis was reached. The canals were obturated with bioceramic sealer using the continuous wave compaction technique, and the tooth was sealed with temporary and then final restoration.
Discussion: The root and root canal morphology of maxillary second molars are known to be more varied than that of maxillary first molars. Untreated or missed root canals can inevitably cause treatment failure; therefore, it is essential to utilize advanced technologies such as cone beam computed tomography (CBCT) and dental microscopes.
Conclusion: Thorough knowledge of the root canal system and its frequent variations is necessary for successful root canal treatment. Future studies should focus on developing educational protocols to train clinicians to recognize and manage rare anatomical variations.
Introduction
The goal of successful endodontic treatment is to clean, shape, and achieve a three-dimensional obturation of the canals. This outcome requires proper knowledge of the complex anatomy of the root canal system of the tooth (1). The root canal system has several variations, rendering achieving a successful endodontic treatment challenging. These variations are detected using cone beam computed tomography (CBCT), periapical radiographs, or microscopic evaluation (1). The normal anatomy of the upper second maxillary molar consists of three roots: a mesiobuccal root, a distobuccal root, and a palatal root (1).
However, there are several variations in the anatomy of the root canal system of the second maxillary molar. It includes six variations: three separate roots and three separate canals (56.9%); three separate roots and four canals, with two canals in the mesiobuccal root, with a percentage of 22.7%; and three roots and three canals, in which the mesiobuccal canal and the distobuccal canal fuse together and form one canal, in addition to the palatal canal (9%) (2). Moreover, the variations in the anatomy of the root canal system of the second maxillary molar include two separate roots with two separate canals, representing 6.9% of second maxillary molars; one main root and one main canal with a prevalence of 3.1%; and four separate roots, each containing its own canal, namely a mesiobuccal root, a distobuccal root, and two separate palatal roots with a prevalence of 1.4% (2).
To detect such a rare variation, multiple radiographs from different angles should be taken. It is preferred that the pre-operative radiographs be digital radiographs, which are useful in detecting calcified and missed canals (3). After detecting the extra canals on the radiographs and achieving access cavity, coronal flaring is preferred to visualize the location of the orifices better. The white line test, where the dentinal walls meet the dentinal floor, can be useful to detect the location of the canal orifices (4). Another useful test is the red line test, in which the remaining blood in vital teeth can help identify the location of the orifices. Ultrasonic devices can be used to locate the canals and deroof it (4). Additionally, troughing using a sharp explorer is beneficial in locating the canal. The champagne bubbling test with sodium hypochlorite can be beneficial in locating extra canals after mechanical preparation (4). Additionally, Loupes and dental operating microscopes can be very beneficial in such complicated cases (5, 6).
Methodology
Case presentation
A 60-year-old male with no medical history presented with a deep carious lesion in the occluso-mesial surface of the left second maxillary molar. A cold test was performed using Endo-ice to test the pulp sensibility, which resulted in a lingering pain. There was no pain on palpation; however, the patient responded to vertical percussion. The preoperative diagnostic radiograph depicted periapical radiolucency surrounding the distobuccal root. Additionally, the diagnostic radiograph showed a variation in the morphology of the number of roots and root canals: four roots, including two palatal roots (Figure 1). A diagnosis of symptomatic irreversible pulpitis and symptomatic apical periodontitis was reached.

Figure 1: Preoperative radiograph showing the morphological variation in the second maxillary molar. The arrows indicate the two separate palatal roots.
Before initiating endodontic treatment, local anaesthesia with 1.8 ml of lidocaine with 1:100,000 epinephrine was administered. Then the tooth was isolated using a rubber dam. A conventional square- shaped outlined access cavity was performed under the dental operating microscope for enhanced visualization, using a round bur size 4 and an access bur. After complete deroofing of the pulp chamber, four canals were located with a DG-16 endodontic explorer. The MB and DB were located in their regular location, in addition to two palatal canals: MP and DP (Figure 2).
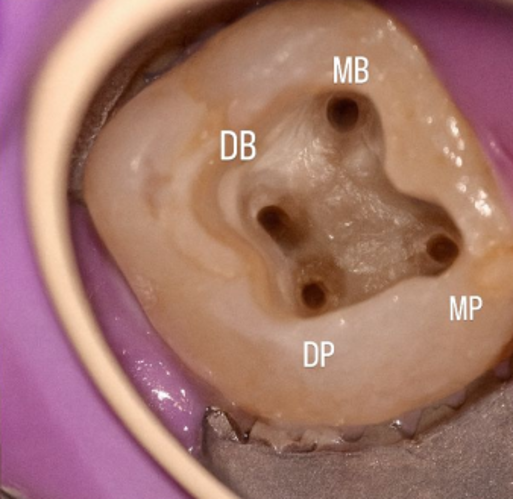
Figure 2: A conventional access cavity after complete deroofing and locating four canals (MB, DB, MP, and DP).
The working length of each canal was determined using an apex locator (Morita Dentaport ZX, Japan), followed by mechanical preparation of the canals up to size 30 with a 0.4 taper using a rotary system (One Reci). The canals were irrigated using 2.5% sodium hypochlorite during the preparation of the canals. The master cones were fitted in the canals and confirmed using a periapical radiograph (Figure 3). Obturation was then performed using a bioceramic sealer and continuous wave compaction technique (Figures 4 and 5).
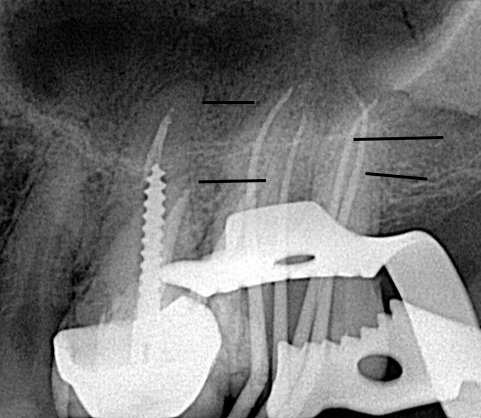
Figure 3: An intraoperative periapical radiograph showing the master cones fit of the four canals.
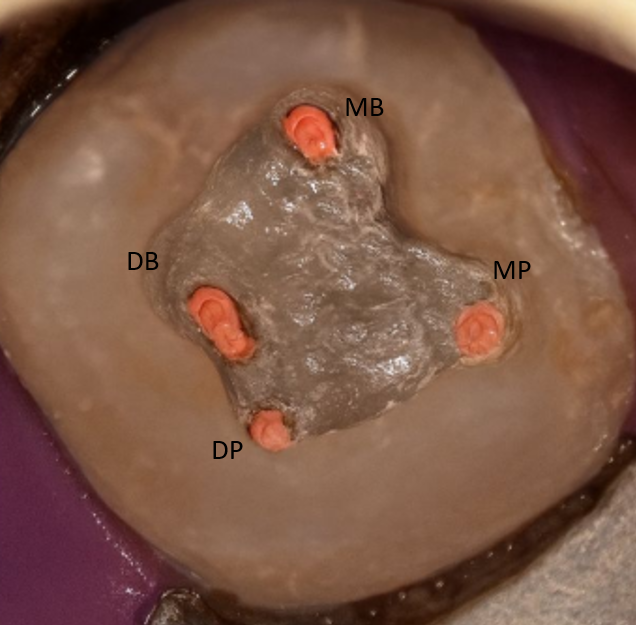
Figure 4: Clinical image showing the obturation of the four canals.
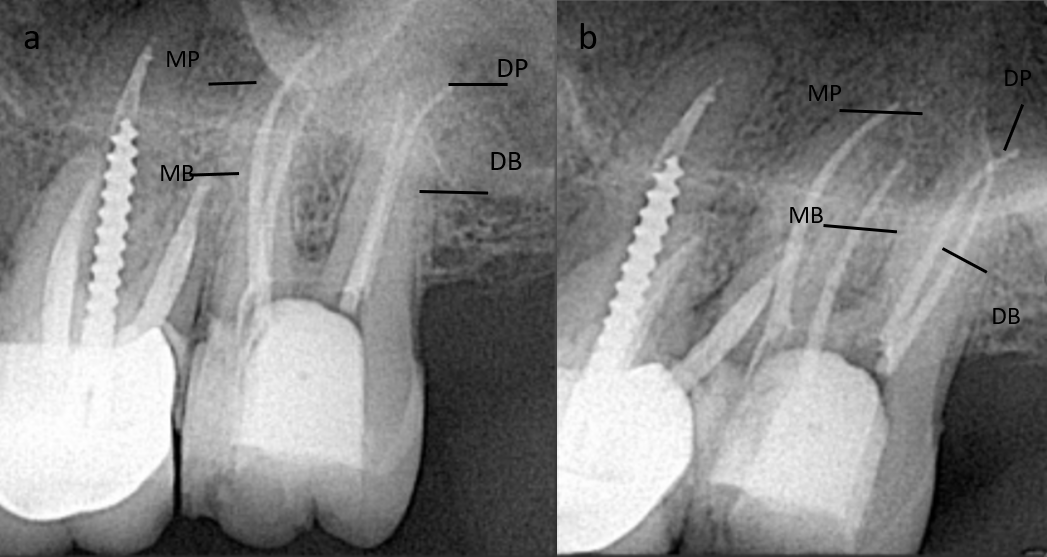
Figure 5: Post-operative periapical radiographs showing the obturation of the four canals with mesial shift (4a) and distal shift (4b).
The canal orifices were sealed immediately postoperatively with a temporary filling and a glass ionomer cement. The final restoration was placed two days after obturation to ensure a proper coronal seal. A CBCT scan was performed postoperatively to verify the presence of two palatal canals and the quality of the root canal treatment (Figure 6).
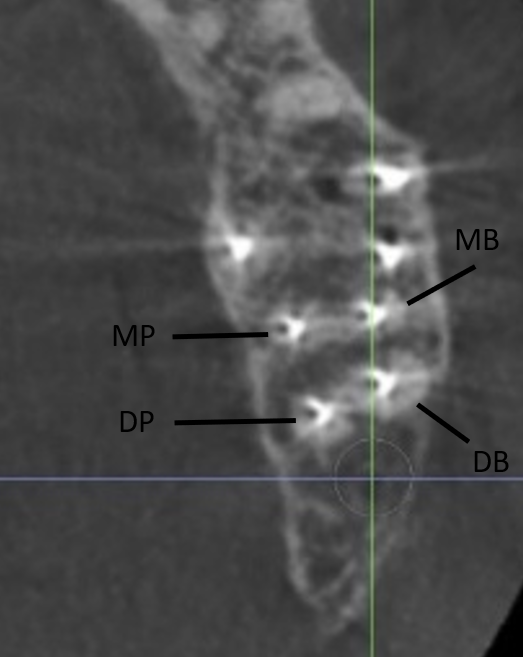
Figure 6: A CBCT scan showing two separate palatal roots (MP and DP) in addition to MB and DB after obturation.
Discussion
Maxillary molars are known for their wide range of canal arrangements. We report a case of a 60-year-old male presenting with a deep carious lesion in the occluso-mesial surface of the left second maxillary molar, whose diagnostic radiograph showed four roots, including two palatal roots. A diagnosis of symptomatic irreversible pulpitis and symptomatic apical periodontitis was reached. The canals were obturated with bioceramic sealer using the continuous wave compaction technique, and the tooth was sealed with temporary and then final restoration. A postoperative CBCT was performed, confirming the presence of two palatal canals and the quality of the root canal treatment.
This root canal variation has been reported by multiple previous case reports (Table 1) (7-15).
|
Table 1. Summary of related studies |
|||||
|
Author |
Patient Age / Sex |
Tooth |
Number of Roots/Canals |
Diagnostic Tools |
Treatment |
|
Alammari 2025 (7) |
40 / Male |
#17 |
4 (2 buccal, 2 palatal)/4 |
CBCT, microscope, radiographs, cold test |
NSRCT with EdgeFileX7, Ca (OH)2, bioceramic sealer |
|
Kottur 2024 (12) |
41 / Female |
#17 |
4 (2 buccal, 2 palatal)/4 |
CBCT, microscope, radiographs, cold test |
Conventional RCT with Protaper Gold, AH Plus sealer, thermoplastic obturation |
|
Matsumoto 2023 (13) |
66 / Male |
Left maxillary 2nd molar |
4 (2 buccal, 2 palatal)/4 |
CBCT, radiographs, 3D printed model, microscope |
Root canal retreatment with NiTi rotary files |
|
Purushotham 2020 (14) |
33 / Male |
#27 |
4 (2 buccal, 2 palatal)/4 |
CBCT, radiographs, microscope |
RCT with WaveOne Gold, saline and NaOCl irrigation, thermoplasticized GP |
|
Al Qahtani 2018 (8) |
35 / Male |
#27 |
4 (2 buccal, 2 palatal)/4 |
Radiographs, microscope |
NSRCT with ProTaper Universal, AH Plus sealer, continuous wave obturation |
|
Alaajam 2017 (case series) (9) |
18–27 / 3 patients (2F, 1M) |
#17/#27 |
4 (2 buccal, 2 palatal)/4 |
Radiographs, apex locator |
RCT with step-back/rotary, calcium hydroxide, thermoplasticized GP |
|
Alenazy 2015 (10) |
45 / Female |
#27 |
4 (2 buccal, 2 palatal)/4 |
Radiographs, microscope |
NSRCT with ProTaper retreatment system, AH Plus sealer, thermoplastic GP |
|
Fakhari 2013 (11) |
45 / Male |
#27 |
4 (2 buccal, 2 palatal)/4 |
Radiographs, clinical examination |
RCT with ProTaper, lateral condensation, AH Plus sealer |
|
Paul 2013 (15) |
32 / Female |
Maxillary 2nd molar |
4 (2 buccal, 2 palatal)/4 |
Radiographs, apex locator |
RCT with crown-down, flexofiles, lateral condensation, AH Plus sealer |
Alammari et al. reported a case of a 40-year-old male patient who was referred to the endodontic clinics at the dental hospital of King Abdulaziz University, Jeddah, Saudi Arabia (7). While our case presented with deep carious lesion in occluso-mesial surfaces of the maxillary left second molar, this patient was referred to evaluating a previously initiated endodontic therapy for the maxillary second molar. The patient presented with intense pain, with clinical examination revealing moderate pain to percussion and palpation, and healthy periodontal pockets. The pathology was found in the apical region of the maxillary second molar, while the pathology of our case was in the apical region of the distobuccal root of the maxillary left second molar (7). A cold test was performed and demonstrated a negative response when compared to other teeth, unlike our case, in which the cold test showed lingering pain. A similar diagnosis of symptomatic apical periodontitis was reached, and a non-surgical root canal retreatment was planned. A pretreatment CBCT was conducted and demonstrated four separate roots and canals. Similar to our case, obturation was performed using a bioceramic sealer but with a different technique (7).
Kottur et al. also reported a similar case of a 41-year-old Indian female patient presenting with pain in her uppermost posterior teeth area for a period of two days (12). The dental examination revealed profound proximal decay and cavitation in the maxillary second molar, with an intact periodontal condition. Similar to our case, percussion elicited a response, and a cold test revealed a tardy response. The patient was diagnosed as symptomatic irreversible pulpitis, which is the same diagnosis of our case (12). Upon radiological assessment, the case presented in this study demonstrated maxillary second molars having four independent roots of two distinct palatal roots. Kottur et al. used a similar establishment method of additional palatal canal to our case, using an operational microscopy and a DG-16 probe. A conventional root canal therapy was performed, followed by a CBCT follow-up. While we used a bioceramic sealer with a continuous wave compaction method, they used an AH Plus sealer and a heated vertical compaction method.
Another case reported by Matsumoto et al. presented with discomfort as a result of the occlusion of his left maxillary second molar (13). Clinical examination revealed percussion pain in the left maxillary second molar. The preoperative diagnostic radiograph revealed periapical radiolucent area in the mesial and distal palatal roots, unlike our case, there was a periapical radiolucency present around the distobuccal root. The patient was diagnosed as having an asymptomatic apical periodontitis of the left maxillary second molar, and root canal retreatment was performed. Like our study, dental CBCT demonstrated four independent roots: mesiobuccal, distobuccal, and two palatal (13).
Multiple root and canal variations in the maxillary molar have been described in the literature. Stone and Stroner have reported two variations in the palatal root of the maxillary molar: firstly, the palatal root may have two canals within a single root, either separated or bifurcated, and secondly, there may be two canals in two distinct palatal roots (16). Afterwards, Christie et al. introduced another classification where the palatal roots were divided into three types: the first type, which is cow-horn-shaped two buccal roots and two long, tortuous, widely divergent palatal roots; the second type, which is four roots that are separate, short, and parallel to each other with blunt apices and separated roots of blunted root apices that run parallel; and the third type, where the root morphology is constricted with mesiobuccal, mesiopalatal, and distopalatal canals engaged in one web of root dentin (17). Furthermore, Peikoff et al. classified variations into six main types: three separate roots and canals, three roots and four canals, two roots with merging canals, two separate roots, a single root, and four roots with two palatal canals (2).
The root and root canal morphology of maxillary second molars are known to be more varied than that of maxillary first molars (18, 19). This can be attributed to the backward position of the maxillary second molar, making it difficult to analyze its inner framework. Untreated or missed root canals can inevitably cause treatment failure; therefore, it is essential to utilize advanced technologies such as CBCT and dental microscopes. CBCT can be used to achieve better visualization by offering detailed three-dimensional views of the root canal system (20). CBCT can visualize additional roots or canals that might be hidden or overlapped in 2D images. This improves diagnostic accuracy and supports better planning and execution of treatments (20).
Strengths and Limitations
Limitations of this study include limited generalizability, lack of postoperative clinical outcomes, and lack of long-term follow-up. Our case report involves multiple strengths, including the documentation of a rare anatomical variation contributing to limited literature, enhanced visualization by using CBCT and a dental operating microscope, and a detailed clinical workflow.
Recommendations
Dentists should consider the morphologic variations of maxillary molars while preparing for any procedure in this region. They should enhance visualization as much as possible by using advanced diagnostic tools, such as CBCT, and by magnification via dental operating microscopes to improve visualization and precision during treatment. Furthermore, advanced irrigation devices should be used for improved debridement of such complex canal anatomy.
Conclusion
This case report documents a rare case of a maxillary second molar with four canals: mesiobuccal and distobuccal canals and two palatal canals, mesiopalatal and distopalatal, that presented with symptomatic irreversible pulpitis and symptomatic apical periodontitis in the left maxillary second molar. Missed and untreated root canals inevitably lead to failure of the treatment. Thus, a thorough knowledge of the root canal system and its frequent variations is necessary for successful root canal treatment. Future studies should focus on developing educational protocols to train clinicians to recognize and manage rare anatomical variations.
Disclosure
Conflict of interest
The author declares no conflict of interest.
Funding
No funding.
Ethical consideration
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Data availability
All data is available within the manuscript.
Author contribution
The author contributed to conceptualizing, data drafting, collection and final writing of the manuscript.
